When Loren Peters arrived in the emergency room in October 2013, bruises covered his frail body, and blood oozed from his gums.
The 85-year-old had not been in a fight or fallen down. Instead, he had been given too much of a popular, decades-old blood thinner that, unmonitored, can turn from a lifesaver into a killer.
“My goodness, I’ve never seen anything like it,” recalled Lorna Finch, Peters’s daughter, of the ugly purple bruise that sprawled from the middle of her father’s stomach to his hip. “It was just awful.”
Peters took Coumadin at his Marshalltown, Iowa, nursing home because he had an abnormal heart rhythm, which increases the risk of stroke. It’s a common precaution, but the drug must be carefully calibrated: too much, and you can bleed uncontrollably; too little, and you can develop life-threatening clots.
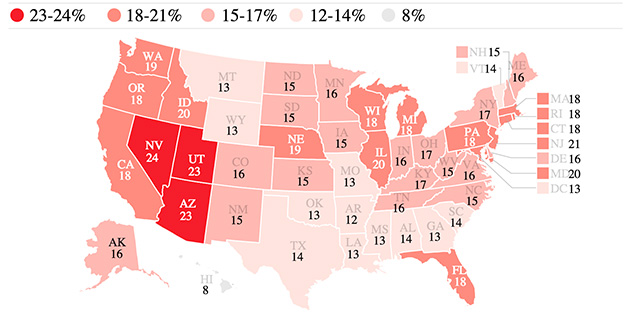
Percentage of nursing home patients receiving at least one dose of anticoagulants per week. Includes Coumadin, warfarin, heparin and other new anticoagulants. Data is for first quarter of 2015. (Graphic by The Washinton Post/source Centers for Medicare and Medicaid Services)
When nursing homes fail to maintain this delicate balance, it puts patients in danger. From 2011 to 2014, at least 165 nursing home residents were hospitalized or died after errors involving Coumadin or its generic version, warfarin, a ProPublica analysis of government inspection reports shows. Studies suggest there are thousands more injuries every year that are never investigated by the government.
“It’s an insidious problem,” said Rod Baird, president of Geriatric Practice Management, a firm that creates electronic health records for physicians working in long-term care facilities. Because it’s so easy to get wrong, “Coumadin is the most dangerous drug in America.”
Nursing homes around the country are routinely cited for lapses that imperil residents, from letting those with dementia wander off to not stopping elders from choking on their food. For years, advocates, researchers and government officials have worried about the overuse of antipsychotic medications that can put elderly patients into a stupor and increase their risk of life-threatening falls. A national initiative helped reduce the use of such drugs among long-term nursing home residents by 20 percent between the end of 2011 and the end of 2014.
But the dangers of the widely used Coumadin have drawn relatively little scrutiny, perhaps because the drug has clear benefits. Still, improper use has caused some patients incalculable suffering and, in some cases, greatly hastened deaths.
Dolores Huss, an 89-year-old grandmother of eight, died from internal bleeding after a San Diego facility gave her an antibiotic that multiplies the effects of Coumadin then didn’t alert her physician that she needed additional blood tests to measure how long it was taking her blood to clot.
Shirley Reim, recovering from hip surgery, was hospitalized with blood clots in her legs after a Minnesota nursing home failed to give her Coumadin for 50 days in a row and also didn’t perform the blood test ordered by her doctor. She suffered permanent damage. Details of the cases come from government inspection reports and lawsuits filed by the patients’ families, which were settled confidentially.
Periodic inspections document hundreds of additional errors that were caught early enough to prevent serious harm, but the real toll is likely much higher, experts say.
Despite such evidence, Coumadin deaths and hospitalizations have drawn only limited attention from the Centers for Medicare and Medicaid Services, the federal agency that regulates nursing homes. Federal officials haven’t tallied Coumadin cases to see the full extent of the damage or identify common problems involving the use of the drug. Neither has the American HealthCare Association, the trade group for nursing homes.
The government investigates incidents like the one involving Peters that trigger complaints or surface in routine inspections. Sometimes, CMS slaps homes with “immediate jeopardy” citations, fining them and threatening to cut off federal funding if quick action isn’t taken. Villa del Sol, where Peters lived, received such a citation related to his care and was fined $33,345.
More commonly, though, homes are not fined and are simply asked to correct the problems and put policies in place to keep them from happening again, ProPublica’s analysis shows.
Last year, the Department of Health and Human Services identified Coumadin and other anticoagulants as one of the drug categories most frequently implicated in “adverse drug events,” calling on government agencies to work on solutions. In a statement, CMS, which is part of HHS, said it is raising awareness of such events, training its inspectors to do a better job at identifying them and working with nursing homes to prevent them.
In Peters’s case, no one at the nursing home conducted the blood test needed to see the effect Coumadin was having, even as bruises spread across his body over a two-week period, government inspectors later found. Peters never recovered, dying a few days after he was brought to the hospital.
Villa del Sol recently changed its name to Hawkeye Care Center Marshalltown. Doug Johnson, president of the home’s parent company, Hawkeye Care Centers, declined to comment by e-mail. “We adhere to privacy rules and practices and do not comment on litigated matters.”
A Breakthrough Drug, With Risks
Coumadin’s roots go back to the 1940s, when scientists at a nonprofit affiliated with the University of Wisconsin at Madison — the Wisconsin Alumni Research Foundation — came up with a rat-and-mouse killer called warfarin, a play off the nonprofit’s initials.
It was derived from a chemical in spoiled sweet clover that had caused cattle to bleed to death after dehorning, castration and other procedures. The substance disrupted the clotting process, so that animals hemorrhaged internally and died.
In the 1950s, drugmaker Endo Laboratories began selling warfarin for human use under the brand name Coumadin. It is in a category of drugs known as anticoagulants. An early user was then-President Dwight D. Eisenhower, who was prescribed the medication after having a heart attack.
Coumadin was a breakthrough for patients with an array of heart troubles associated with blood clots. These include abnormal heart rhythms, along with pulmonary embolisms and deep vein thrombosis.
But the drug interacts badly with certain foods and medications, particularly antibiotics, and it requires regular blood tests to ensure it’s working as intended. The test measures the time it takes for blood plasma to clot.
In Medicare’s prescription drug program, known as Part D, 2.4 million seniors and disabled people filled at least one prescription for warfarin, the generic of Coumadin, in 2013, making it one of the most-used drugs. About 280,000 were prescribed brand-name versions, Coumadin and Jantoven. Many people, including health inspectors, continue to call the generic versions Coumadin because it is so well known.
About 1 in 6 of the nation’s 1.3 million nursing home residents take an anticoagulant, according to federal data from earlier this year; the majority are believed to be on Coumadin or its generic.
Newer anticoagulants, including Eliquis, Pradaxa and Xarelto, have entered the market in recent years and, in some ways, are easier to use than Coumadin. Patients taking these drugs don’t need regular blood tests and don’t have to avoid certain foods.
But unlike Coumadin, the effects of which can be reversed with vitamin K, there currently is no antidote if patients taking the newer drugs begin bleeding uncontrollably.
Some doctors also are reluctant to use the new drugs on seniors, particularly those with multiple health problems, because they carry their own risks, including gastrointestinal bleeding.
‘Perfect Setup for Bad Things’
Coumadin is tricky to manage even for otherwise healthy patients who don’t live in nursing homes. A study published last year by the lab company Quest Diagnostics found that patients taking Coumadin or its generic had lab results showing that the drugs had the desired effect only 54 percent of the time.
A 2011 report in the New England Journal of Medicine found that the drug accounted for some 33,000 emergency hospitalizations among the elderly from 2007 to 2009, more than twice as many as the next highest drug, insulin. The study did not look exclusively at nursing home residents.
Given Coumadin’s challenges — and the coordination required among doctors, nurses, pharmacists and laboratories – nursing homes are the “perfect setup for bad things happening,” said Jerry Gurwitz, chief of geriatric medicine at the University of Massachusetts Medical School. Since the 1990s, when he first wrote about the problems of Coumadin in nursing homes, “very little, unfortunately, has changed,” he said.
Federal inspection reports repeatedly cite the same types of problems: patients not getting the drug as ordered, or given the wrong doses, or given without a doctor’s order.
A Texas nursing home resident received Coumadin for 34 days “without a physician order or adequate monitoring.” Blood was pooling in his mouth when he was sent to the hospital. A patient at a Minnesota home needed three surgeries for a blood clot in the left leg after not receiving 17 doses of the medication.
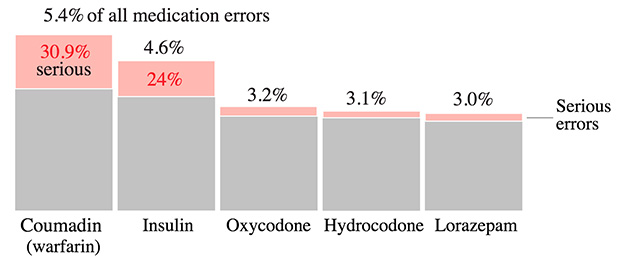
The drug most commonly involved in nursing-home medication errors also presents the highest rate of serious errors. Top five drugs of numerous medicines cited; data from fiscal year 2012. (Graphic by The Washinton Post/source Medication Error Quality Initiative)
Failure to monitor the drug can lead to dangerous side effects. At a North Carolina home, a patient on Coumadin wound up in the hospital after no clotting tests were done for a month. An internal review found that a nurse “mistakenly put the February labs on the wrong month.”
Sometimes, the tests were done, but nursing homes didn’t alert doctors when the results were abnormal. At a Maine nursing home, a doctor wasn’t told when lab results showed a resident’s blood took too long to clot. Days later, when staff assisted the resident to the bathroom, the resident passed out and had no heartbeat. It is unclear if the resident survived.
In several cases, patients taking Coumadin fell, and nursing homes were cited for not doing enough afterward to ensure their safety. In Arkansas, a resident on the drug fell and hit his head during exercise class. A nurse said she didn’t call his doctor because the doctor “didn’t like to be called at night unless it was an emergency.” The resident died from the consequences of massive bleeding in the brain.
Vigilance Difficult to Enforce
Most patients who are taking Coumadin need it, experts agree. But problems with monitoring occur even at facilities trying to be vigilant.
A report published last year in The Consultant Pharmacist journal found that 12 New York nursing homes given tools to improve how they handled patients on Coumadin — including staff education programs — largely failed to improve their management of the drug.
“Improvements were not seen despite active intervention,” the report’s authors wrote. “If long-term care facilities are unable to voluntarily implement necessary improvements, then regulatory changes may be necessary to assure patient safety regarding anticoagulant use.”
David Gifford, senior vice president of quality and regulatory affairs at the American Health Care Association, said Coumadin errors can’t be viewed in isolation. “Those that approach one area at a time, they’re chasing their tail and they’re not going to see improvements,” he said. “This week, the soup du jour is Coumadin errors … then next week, it’s insulin errors.”
The association recently announced a quality initiative aimed at, among other things, reducing “unintended health care outcomes” — a broad category that covers various types of errors, including those involving medication.
Some long-term care associations say it would be better for CMS to work with the nursing home industry to change its practices rather than to take each incident in isolation, using citations and other sanctions to bring homes in line. Another concern is not to discourage doctors from prescribing Coumadin.
“It may be distorting a little bit to look at the immediate jeopardy outcomes [cited by regulators] without looking at the overall population that’s on it and needs to be on it,” said Cheryl Phillips, senior vice president of public policy and advocacy at LeadingAge, an association of nonprofit senior service organizations. “In fact, to not put people on blood thinners is a huge risk and in many cases malpractice.”
‘Things Didn’t Get Any Better’
Peters, a retired factory worker, moved into Villa del Sol in 2011 with his wife of more than 60 years, Arleta, who had fallen and could no longer walk on her own.
In September 2013, during a weeklong hospital stay, Peters was diagnosed with a variety of abnormal heart rhythms and sent back to the nursing home on Coumadin, the government’s inspection report said.
Both the hospital and Peters’s doctor left instructions for the nursing home to give him a particular test to assess his clotting rate. But it was never done. Instead, the staff gave him a different test intended for patients taking heparin, another blood thinner.
One nurse told inspectors that “it never occurred to her to look to see if the blood work was for what the physician ordered.” Another said “it never occurred to her that this resident was on Coumadin” and needed his blood monitored, according to the government report.
In the first two weeks of October, staff members made several notes in Peters’s chart about bruises on his body. Several entries mentioned scattered bruising; one noted a large bruise on the right abdomen that was purple in the center, green and yellow on the outside. The nurses decided among themselves that the bruises must have been from the lift they used to transfer him, the inspection report said.
Peters was taken to the emergency room after midnight on Oct. 15, 2013, because of the bleeding from his gums. There, a quick test showed that his blood took so long to clot that he might never stop bleeding on his own — a result his doctor told inspectors she’d never seen before.
The doctor later told an inspector that Peters’s bruises were so “horrible” she asked the hospital to take pictures of them. (Photos were taken, said Jeffrey Pitman, an attorney for Peters’s family.)
“They had to have noticed the bruises, and why didn’t they do something about it?” said Finch, Peters’s daughter, who is considering a lawsuit against the home.
At the hospital, doctors gave Peters vitamin K to try to counteract the Coumadin.
He grew confused, agitated, almost belligerent. He had trouble breathing.
“It just got to a point where things didn’t get any better,” said Finch, 59. “I asked his doctor: ‘What really is going on here? Do we have any hope of getting Dad back?’ [The doctor] said, ‘You know he’s pretty weak.'”
As hopes for Peters faded, his wife, too, became ill and was taken to the same hospital. Peters’s family decided to move him to his wife’s room so they could be together for his final hours.
When Peters was wheeled into the room, he was “pretty much unresponsive,” inspectors wrote. “However, when they put [his] spouse’s hands in [his], the resident woke up and was able to talk.”
He died the next morning; Arleta, three weeks later.
“When Dad passed away, she quit,” Finch said. “She just broke down and she screamed, ‘I am so mad at him, he didn’t take me with him.'”
Scenes from Advair’s Las Vegas launch. (Image courtesy of ProPublica)
Advair is one of the biggest blockbusters in pharmaceutical history.
The asthma drug has generated more than $80 billion in global revenues for its maker, GlaxoSmithKline, since its U.S. approval in 2000. With its distinctive purple inhaler, Advair has helped legions of asthma sufferers achieve control of their symptoms.
But recent federal research suggests that a significant percentage of asthma patients begin using Advair inappropriately, taking on what the drug’s label describes as an increased “risk of asthma-related death” from one of its two ingredients.
Concerns about that ingredient — salmeterol — emerged in a 1993 study, and more troubling results became known in early 2003. But it took the Food and Drug Administration seven more years to require Glaxo and makers of drugs similar to Advair to launch studies big enough to assess the risks.
Results aren’t due until 2017. Meantime, millions of patients on the drugs — a class long dominated by Advair — remain exposed.
Portions of Advair’s story have been told before, but a ProPublica examination, based on previously undisclosed or overlooked documents, shows that the traditional guardians of U.S. drug safety — manufacturers, regulators, doctors and the courts — have repeatedly failed to stop misuse of Advair or unlock its secrets.
Before Advair’s approval, a Glaxo scientist told the FDA that it wasn’t appropriate for patients with mild asthma. The agency agreed, a Glaxo document states, but it took five years to make that clear on the drug’s label.
When a handful of state Medicaid agencies moved to limit access to Advair, based on concerns about misuse, Glaxo lobbied aggressively to stop what was viewed internally as an “infestation” of such policies.
And Glaxo has faced scores of lawsuits and claims brought by people whose relatives have died while taking Advair, quietly settling some when pushed to the brink of disclosing sensitive documents.
Through it all, Glaxo’s muscular Advair marketing machine, abetted by broad doctor and patient support, has continued to chalk up huge sales.
Glaxo paid $700 million in 2012 to settle federal civil allegations that unlawful promotion of Advair contributed to extensive misuse, but regulators reported last year that overutilization remained a problem even after more urgent warnings to doctors and patients in 2010.
Glaxo vigorously denied the false-marketing claims brought by the Justice Department. The British-based company said it has changed its practices by ending certain financial payments to doctors and eliminating targets for sales reps. Its marketing policies, for Advair and other drugs, have always required that the company follow FDA rules, Glaxo said in a statement.
The company said Advair is safe when used properly and that dozens of studies have shown its “positive safety profile” and superiority to other asthma treatments. There have been no asthma-related deaths in more than 15 years of Advair trials involving 30,000 patients, Glaxo said.
“We are proud to be in the forefront of research and development in the respiratory field and to have helped millions of patients with asthma,” the company said, adding that patients could suffer if they stopped taking Advair because of too much emphasis on risk.
The FDA said in a statement that Advair “was approved more than a decade ago based on evidence that supported its safety and efficacy.” Although it later required warnings and new trials, the agency said it still believes the benefits of Advair and similar drugs are substantial.
Some 3,500 people die from asthma every year in the United States. Although no deaths have been definitively linked to Advair, in 2003 Glaxo shut down a study of salmeterol earlier than originally intended after 13 patients died.
An FDA scientist later summarized the results: one excess asthma death for every 1,300 users of salmeterol. A prominent FDA epidemiologist, Dr. David Graham, even called for Advair and similar drugs to be banned for treating asthma, calling their ongoing use a “natural experiment.”
But Graham was in a distinct minority; others in the agency said that Advair’s benefits outweighed any risks, which could be managed.
That was also the predominant view among asthma specialists and researchers — although a few broke from the pack. Within the latter group was Dr. Fernando Martinez, a prolific asthma researcher who runs a top respiratory center at the University of Arizona.
Martinez helped lead calls for the large-scale trials the FDA eventually required for Advair and similar drugs. His center treats thousands of patients, and as a youth he watched his mother suffer with the disease.
Martinez felt that Advair was appropriate for many patients. But he was also concerned about the consequences of over-medicating and felt the need to speak out.
Without answers from the ongoing safety trials, he said in an interview, “You are putting at risk people who do not even need the medicine.”
A ‘Very Successful’ Label
Asthma is among the most common chronic diseases in the world, affecting roughly 25 million Americans, including 7 million children.
It causes sufferers’ airways to narrow and become inflamed, impairing breathing and causing bouts of wheezing, gasping and sleepless nights.
Some patients, about 35 percent, have only intermittent symptoms, according to the Centers for Disease Control and Prevention. Those with persistent asthma can be diagnosed as mild, moderate or severe.
There is no cure. Overall, asthma deaths are relatively rare. They declined from 2001 through 2009, according to the CDC, but have subsequently nudged upward. More than 400,000 people are hospitalized in the United States each year for acute attacks.
Before Advair, patients often had to juggle more than one medication to keep their symptoms in check. Studies show that many asthma sufferers didn’t follow their doctors’ orders and ended up undertreated.
Advair was designed to address those problems. It combined two established ingredients — a corticosteroid to reduce inflammation and salmeterol to open airways — in one simple inhaler.
Advair’s two main components had each previously undergone clinical trials to prove their safety and efficacy before winning regulatory approval. Still, questions arose about the safety of salmeterol, one in a class of asthma medications called long-acting beta-agonists, or LABAs.
A 1993 study found that patients in the United Kingdom taking Glaxo’s salmeterol-only drug, Serevent, had a higher rate of asthma mortality, although the finding wasn’t statistically significant. The FDA approved Serevent, but when reports of asthma deaths came in soon after, Glaxo began a large-scale safety study.
That research was still in progress in 1999, when Advair came up for approval. Glaxo submitted results from small trials that showed its combination drug was effective and had no serious adverse effects.
The FDA also had to consider which patients should get the drug and how to describe the appropriate population under the “usage” section of Advair’s label.
The issue arose at a 1999 meeting of experts the FDA had convened to seek advice about the label and other matters. For those with only “mild asthma” controlled by a single medication, the “combination therapy would be inappropriate,” Dr. Tushar Shah, then Glaxo’s director of respiratory clinical research, stated at the session.
Yet the language Glaxo proposed for Advair’s label wasn’t nearly as direct — it did not specifically rule out mild asthma. Particularly for family physicians and other non-specialists, it offered “a fairly vague statement,” observed Dr. Michael Niederman, chief of pulmonology at Winthrop-University Hospital in Mineola, New York.
Dr. Robert Meyer, then director of the FDA’s pulmonary division, agreed with Niederman, but others argued that physicians needed flexibility. Meyer cautioned that it wasn’t the FDA’s role “to be either tacitly endorsing or restricting the practice of medicine.”
He said the FDA hoped to work with Glaxo “to perhaps better define the population” of patients for Advair. When the agency’s medical review was completed in January 2000, the author wrote that the FDA would revise Advair’s package insert to “clarify” the matter.
That August, the FDA approved Advair as generally safe and effective. But the label’s “usage” section simply said Advair was for “maintenance treatment of asthma in patients 12 years of age and older.”
Inside Glaxo, officials were aware that the “FDA is not comfortable that Advair be used or promoted for mild disease,” according to a company memo written on the eve of the FDA’s decision.
On an April day in 2001, more than 2,000 Glaxo salespeople flocked to the Paris Las Vegas hotel for events to launch Advair. Spotlights swirled and the room glowed purple, matching a giant replica of the drug’s inhaler.
Jim Daly, the Glaxo manager nicknamed “Mr. Advair,” took the stage sporting a purple tie. “There are people in this room who are going to make an ungodly sum of money selling Advair,” he told the cheering throng.
The 50 salespeople who persuaded physicians to prescribe the most Advair would get $10,000 bonuses on top of healthy commissions.
“I think we can make some millionaires out there,” declared Glaxo’s then-president of pharmaceutical operations, David Stout.
Stan Hull, the company’s senior vice president at the time, rhetorically asked the crowd, “What patient is not appropriate for Advair?”
According to the label’s “usage” language, virtually all asthmatics over 12 were potential Advair customers. Yet treatment guidelines generally called for starting patients with mild or intermittent asthma on other drugs, such as Glaxo’s Flovent, the steroid component of Advair.
Glaxo had strong incentive to prefer patients get its new drug — Advair sold for much more. (Currently, it can cost more than $300 a month, about 50 percent more than Flovent.)
Despite its higher price, Advair won over doctors and patients almost immediately, surpassing even the ambitious sales goals set in Las Vegas. Some 10 million prescriptions were dispensed in the drug’s introductory year. In 2002, Advair amassed $1.4 billion in sales.
One of those early prescriptions went to Lisa Wade, an athletic high schooler who lived in the rural town of Leesport, Pennsylvania.
Lisa’s symptoms had included a few serious asthma attacks a year — “not that bad,” according to her father, Jeff, who managed computers at a bank.
“The selling point was convenience,” said her mother, Mary Kay, an emergency room nurse.
For several months after Lisa started Advair, her symptoms stayed about the same. But beginning in the spring of 2002, her flare-ups increased in severity and frequency, scaring her family.
On the night of Sept. 17, Lisa was home alone, filling out a college application on her computer, when a serious attack struck. She managed to call 911 before collapsing. It took the ambulance just four minutes to arrive, but Lisa couldn’t be revived.
Mary Kay was on duty at the ER when they brought in her daughter. Just past midnight, doctors pronounced Lisa dead. It was three weeks after her 17th birthday.
In their grief, the Wades set about researching Advair. Spurred by a news article, Mary Kay learned about studies linking salmeterol with an increased risk of death. She called the FDA, which collects reports on bad drug reactions, to explain what happened to Lisa, saying she’d heard about 12 similar deaths.
“The guy said to me, ‘I guess your daughter just made it 13,’ ” Mary Kay recalled.
The Wades sued Glaxo for wrongful death in Philadelphia’s common pleas court. The company denied liability.
As part of the litigation, Lisa’s body was exhumed and autopsied, but even that didn’t bring certainty about the cause of death. The report, by a forensic pathologist, concluded Lisa died of “acute cardiac arrhythmia and heart failure due to complications of bronchial asthma or its therapy.”
In a statement to ProPublica, Glaxo said, “We are prohibited from discussing any specific patient, his or her asthma condition, prescription drug use and a host of other critical factors that may be useful in evaluating medical causation and alternative medical causation.”
The Wades’ case was settled confidentially.
A Call To ‘Clear the Air’ About Excess Deaths
As the Wades sought answers about their daughter, the asthma community got a jolt. Glaxo halted its salmeterol safety trial earlier than expected.
Begun in 1996, the study was known by the acronym SMART and had become the biggest asthma drug trial ever conducted, involving 26,000 patients. But after 13 patients on salmeterol died and participation flagged, the study’s safety board recommended either enrolling more patients or closing it down.
In January 2003, Glaxo ended the trial and notified the public and health-care providers of the results: The rate of asthma-related death for patients on salmeterol was four times higher than for patients on a placebo.
To Arizona researcher Martinez, the demise of SMART struck like a “lightning bolt.” He had started out as an Advair fan, “happy with the medicine,” as he put it. Although Martinez still believed Advair was the best choice for some patients, the salmeterol risk was troubling.
Compounding the issue, Glaxo’s initial analysis of the SMART results made the numbers look better than they were.
Without telling the FDA, the company included patient outcomes that occurred up to six months after the study period ended. The effect was to boost the number of asthma deaths for patients on placebos, shrinking the gap with salmeterol.
The FDA noticed, and Glaxo had to resubmit its results. The agency later called the initial analysis “artificial.”
In a statement about the matter, the company said it “actively communicated the outcomes to regulatory bodies and other stakeholders, and the information was promptly made public.”
Within months, the FDA approved new warnings for packaging on all LABA drugs, including Advair.
By early 2005, the SMART study was still being widely debated in the asthma community. The FDA invited Martinez and other experts to help decide what to do next.
In private discussions with the FDA, Glaxo had argued that the steroid ingredient in Advair ameliorated the risk of the salmeterol compound. The agency had rejected that contention as unproved.
That July, the agency convened its Pulmonary-Allergy Drugs Advisory Committee to consider whether additional warnings were needed.
As the discussion unfolded, one panelist — David A. Schoenfeld,a Harvard professor of medicine and statistics — calculated the risk of death for salmeterol users, based on SMART. He put it at one excess death for every 700 patients with a year of exposure.
The figure alarmed members of Glaxo’s team, who worried that the estimate “might appear in the public domain without appropriate caveats” and be a “disservice to patients.” Instead, the company cited studies where it didn’t “see an attributable risk of that sort.”
A company presenter, Dr. Katherine Knobil, said there were too few deaths during SMART to provide “any clear explanation of the results.”
Martinez acknowledged Glaxo’s theory that Advair’s steroid ingredient might offset the risk of salmeterol. But he said SMART wasn’t designed to answer that question. “I do not think that the data, as I see it today, justifies saying that this risk is decreased by steroids,” he told the group.
Instead, Martinez suspected drugs like salmeterol might be backfiring in a small population of patients, including those with rare genetic variations. For that population, “the main expression of the disease is severe attacks that are not only not controlled by these medications,” he said, “but may be rendered worse” by them.
Martinez came away convinced that the answer was more research — and that the drug makers should be digging deeper.
That December, he took the unusual step of publishing an essay in the New England Journal of Medicine. “Until the manufacturers of these drugs undertake the appropriate studies needed to clear the air,” Martinez wrote, the safety of drugs like Advair “will remain uncertain.”
Doctors ‘Aren’t Going to Listen’ to the FDA
The FDA did not order studies. But the month before Martinez’s article appeared, the agency did revisit Advair’s broadly worded label.
In late 2005, the drug regulator required new “usage” language saying “physicians should only prescribe” the drug to patients whose asthma wasn’t already controlled by inhalers like Flovent, or whose asthma “clearly warrants” more than one medication.
Publicly, Glaxo executives shrugged. Although manufacturers can’t promote drugs for off-label use, doctors are free to prescribe them as they see fit.
The revised label “is not going to have a big effect” on Glaxo’s blockbuster drug, CEO Jean-Pierre Garnier told Wall Street analysts in January 2006. Doctors, he said, “are not going to listen to the FDA.”
Inside Glaxo, executives weren’t as sanguine.
The company’s marketers had been targeting “high volume Medicaid” doctors to boost Advair sales, according to documents in the Justice Department case that were unsealed at ProPublica’s request.
A top company executive had even boasted about the results in a briefing for investors, the documents show.
After the FDA’s label changes, though, Medicaid officials in Arkansas moved to limit access to the drug. A state analysis confirmed that most Medicaid patients with mild cases of asthma were getting Advair despite treatment guidelines saying they shouldn’t.
“People were being treated with the most expensive, the most risky combination, jumping right to the top of the mountain with no evidence they needed it,” said Dr. Mark Helm, who headed the Arkansas study.
Arkansas’ Medicaid program started requiring doctors to get prior approval before prescribing Advair. The change dramatically cut prescriptions without adverse health consequences to patients, Helm said.
But when Helm and his colleagues began sharing their approach with Medicaid officials in other states, Glaxo launched a counteroffensive to make sure that what happened in Arkansas stayed in Arkansas.
After Ohio proposed restrictions, a company lobbyist reported testimony from a doctor who called them an “unnecessary burden” that would be “dangerous for patients,” an April 2007 email chain shows.
Ohio ultimately adopted limits, but the company’s opposition strung out the debate for an additional three months. The delay was valuable enough to Glaxo that executives nominated those involved for “Spirit Awards,” according to one of the company emails.
After a few years, only eight states restricted Advair in Medicaid.
Responding to questions about lobbying, Glaxo said in a statement that it has worked with many states to “assure the availability” of drugs, including Advair, and that it disagrees with efforts that “deny treatment to appropriate patients as recommended in national guidelines.”
In the Courts, A Fight Over Disclosure
Glaxo fended off one threat. Now its lawyers grappled with another: A growing stack of lawsuits had been filed against the company blaming Advair for deaths or harm from severe asthma attacks.
In the summer of 2006, a case in rural Alabama took on added importance as plaintiffs’ attorneys pushed for the disclosure of a cache of internal Glaxo documents about Advair.
The plaintiff was an Alabama truck driver named Earl Faulk, who contended that the death of his 20-year-old son, Marcus, was linked to use of Advair and Serevent.
The company’s attorneys resisted Faulk’s demand for documents, saying Glaxo had already released more than 1 million pages. The additional documents included private communications between the company and its attorneys and should not have to be turned over, they argued.
The decision fell to Christina Crow, a lawyer engaged as a special master by the judge presiding over the case.
Crow questioned Glaxo’s claim of attorney-client privilege. The documents “weren’t seeking advice,” she said in an interview. “They seemed to be copying an attorney just so privilege could be invoked.”
Crow ordered the company to hand over more than 100 documents. Before the records could change hands, however, Glaxo and the Faulks resolved the case confidentially.
Other cases also ended abruptly after lawyers sought the same cache of documents, according to one plaintiff’s lawyer, Lynn Seithel. A former Republican legislator in South Carolina, Seithel estimates she “worked on about 250 cases” involving Advair. None went to trial, records show.
As in the Wades’ lawsuit, Glaxo denied liability and said it could not comment about the cases or their resolution.
Crow may be the only person outside Glaxo or its attorneys to have seen the documents Faulk sought.
“I learned a lot about asthma and Advair,” Crow said. While she is prohibited from disclosing what they say, Crow said it was a relief that members of her family “don’t have the disease or take the medicine.”
‘How Can We Justify Exposing Millions?’
The legal settlements kept some of Advair’s secrets out of view, but they didn’t diminish the debate over its safety.
In December 2008, the dispute spilled out into full view when FDA scientists split over whether Advair should still be approved to treat asthma. The agency declined to make officials available for interviews.
Martinez was in attendance as the FDA convened three different advisory groups to discuss what to do about long-acting beta-agonists like salmeterol, the Advair ingredient linked to asthma deaths.
With more than 3 million asthma users, Advair dominated all combination LABA drugs. The medications are also used to treat chronic obstructive pulmonary disease (COPD), but an increased mortality risk hasn’t been demonstrated for COPD.
The FDA’s Dr. Andrew Mosholder recounted the findings from SMART, the study Glaxo had shut down five years earlier: Salmeterol was linked to one excess asthma death for every 1,300 patients in the 28-week trial. Expressed in terms of a full year, that is the equivalent of the one-in-700 estimate that Harvard’s Schoenfeld cited in 2005.
Graham, part of a surveillance and epidemiological team with Mosholder and others, said there was no evidence the risks for Advair weren’t as high or worse. Taking on his agency, he said the FDA should have ordered Glaxo to do a large safety trial “many, many years ago.” The company “apparently didn’t volunteer” to do one either, he noted.
“How can we justify exposing millions to what we must conclude is an extremely high risk of death?” Graham said, referring to Advair and other combination LABA products.
He and Mosholder couldn’t, Graham said. The two recommended that the FDA no longer endorse the drugs for asthma care.
The stance put them at odds with the FDA’s pulmonary experts. Dr. Badrul Chowdhury, head of the agency’s pulmonary division, countered that taking Advair away could make things worse.
Chowdhury said asthma deaths had trended down since Advair hit the market. Patients might turn to less-effective drugs or make more frequent use of rescue inhalers, which also carry a mortality risk, he said.
“This shift will not reduce mortality, but may increase it,” Chowdhury said. He also cited an FDA meta-analysis of multiple studies that collectively suggested Advair was safer than other LABA drugs. Any risks can be managed with appropriate labeling, he said.
In a statement to ProPublica, Glaxo said excess asthma deaths like those seen in the SMART study “would have suggested a significant increase in asthma fatalities rather than the observed decline” in recent years.
Advair supporters — from families with asthma-stricken kids to physicians — also defended the drug at the FDA meeting.
Ultimately, the advisers went with Chowdury. Martinez joined a unanimous vote affirming that Advair’s benefits outweighed any risks in adults. By a narrow margin, the group also backed continued use by children.
Four months later, another influential voice entered the debate.
Dr. Jeffrey Drazen was both editor-in-chief of the New England Journal of Medicine and a veteran asthma researcher at Harvard Medical School. Years of inaction on the issue of LABA safety studies disappointed him.
In an editorial, Drazen and a co-author from Canada wrote that if drug makers didn’t launch new trials to address the matter, the FDA should force them to do so. “As members of a community of physicians, we must demand that such studies be done, be done soon, and be done correctly,” the two wrote.
With sales of Advair and similar drugs topping $6 billion a year, even a big trial would cost the equivalent of only a couple of weeks of profits, they said.
It took nearly a year for the FDA to move.
In February of 2010, the agency required Glaxo and three other manufacturers to conduct studies large enough to measure the risk of asthma death and life-threatening hospitalizations for their drugs.
Advair had been on the market for almost a decade. Utilization studies confirmed what Helm found in Arkansas — that Advair was being prescribed inappropriately to most of the patients who got it.
The FDA initiative included stronger language on the drugs’ labels, emphasizing that they should only be prescribed if other therapies were inadequate and that they should be discontinued as soon as possible.
Marketing and ‘Massive Overutilization’
While the FDA’s regulators moved forward, its investigators began working with federal prosecutors on a probe that had Glaxo and Advair quietly in its crosshairs.
Years earlier, current and former Glaxo sales reps had filed lawsuits under the U.S. False Claims Act, alleging the company had unlawfully marketed several of its drugs and defrauded federal health programs.
The Justice Department eventually joined the cases, providing the plaintiffs access to millions of records subpoenaed from Glaxo.
Initially, the case had focused on other Glaxo products. But in 2009, at a meeting with government prosecutors in Boston, the whistleblowers’ lawyers laid out evidence that Glaxo marketed Advair to mild asthmatics, despite knowing it might not be appropriate, court documents show.
In 2011, the Justice Department filed — still under seal — a civil fraud complaint alleging, among other things, that Glaxo had unlawfully promoted Advair, exposing patients to “significant safety risks without demonstrated treatment benefits.”
The result was ” massive overutilization of Advair” by people who, according to federal treatment guidelines, shouldn’t have been taking it, the government’s case alleged.
Relying in part on the subpoenaed Glaxo documents, the complaint estimated the misuse at between 50 percent and 90 percent. Moreover, Glaxo had promoted Advair over its less-expensive Flovent, even when Flovent was medically appropriate, the government said.
The allegations didn’t become public until the summer of 2012, when the government and Glaxo settled. Although Glaxo denied wrongdoing with regard to Advair, the company agreed to pay more than $700 million related to the drug, part of a $3 billion deal involving eight medications.
“The settlement was a way to resolve the government’s allegations and move forward,” the company told ProPublica.
Glaxo also agreed to reform its marketing practices. It changed bonus arrangements for its sales force in 2011 and last year committed to end the practice of paying doctors to speak on behalf of its drugs. “We’ve taken responsibility for past conduct, learned from our mistakes and have changed as a company,” Glaxo said in a statement.
News accounts of the July 2012 settlement focused mostly on Glaxo’s other drugs, rather than Advair, which largely retained its halo among doctors and patients. Sales exceeded $4 billion in the United States that year, more than five times what Glaxo paid to resolve the government claims.
A Genetic Clue, Years After A Pitch
The FDA-ordered safety trials began in 2011, and Glaxo said it is “working diligently” to meet the agency’s mandate.
In response to critics like Drazen, Martinez and Graham, who say the company should have initiated a trial, Glaxo said in a statement that none of the drug makers doing studies had done so as they “awaited the direction” of the FDA.
Glaxo said there have been no asthma deaths in the trial. The company also said results for adult and adolescent subgroups should be ready this fall, which would make Glaxo the first to report its findings. A separate pediatric study is expected to be completed ahead of the FDA deadline, the company said.
As part of the trial, Glaxo said it collected genetic data for further research, even though the FDA did not require it.
Eight years ago, however, the company passed up a chance to pursue a line of genetic research that has since proved fruitful.
In 2007, Glaxo sent Martinez an email inquiring about his interest in investigating whether genetics might explain severe asthma attacks in patients taking LABA drugs. Martinez wrote back, asking “how seriously GSK [Glaxo] would want to pursue these issues.”
He proposed a study of rare gene variants, saying it could put Glaxo “at the forefront of severe asthma genetics,” according to emails obtained under Arizona public records law. Glaxo scientist Steve Yancey later visited Tucson to meet Martinez, who was paid a small consulting fee.
Glaxo and Martinez never teamed up. But last year, Lancet Respiratory Medicine, an arm of the prestigious British medical journal, published a study that was essentially the same as the one Martinez had proposed.
The authors found that patients with rare genetic variations who took a LABA drug had twice the rate of asthma-related hospitalizations and a higher incidence of asthma attacks.
American taxpayers financed the research through federal grants.
Asked why Glaxo didn’t follow up with Martinez, the company said it lacked a sufficient genetic database at the time. Glaxo said it now has enough data for its own study and expects results this fall.
Misuse of Advair and other drugs with long-acting beta-agonists persists, according to a team of FDA and independent researchers.
Their lengthy, little-noticed study, released in January 2014, examined the effect of the label changes and patient guides the FDA mandated in 2010. It found little or no impact: The portion of patients who inappropriately started taking LABAs held at about 27 percent. The length of time patients used the drugs didn’t budge, either.
The findings came two years after Glaxo sent the FDA its own utilization study, contending that a decline in Advair prescriptions between 2005 and 2011 demonstrated that its safety communications were working.
Martinez noted that the biggest declines were in pediatric dispensing, while adults accounted for more than 80 percent of Advair users in Glaxo’s study.
In an email, Glaxo criticized the FDA’s study because it relied on insurance claims data, which don’t reflect asthma severity or other factors a doctor might consider when prescribing Advair. “It is the physician who is best suited for making the correct decision about which therapy to initiate for a patient,” the company said.
About one out of every six Americans with asthma takes Advair or a similar drug, according to the FDA study. Although competitors have taken some of Advair’s market share, with sales dipping to $3 billion last year, it remains the top-selling combination asthma medicine.
Drazen, the Harvard asthma expert, said doctors remain loyal to Advair because they see patients get better. “One of the reasons it’s hard to convince lung doctors of the risk is that the drug is so effective,” he said.
A few who’ve been affected by Advair need no convincing about risks.
Tim and Sarah Passons’ daughter, Brennan, was a straight-A student at Queen of Angels Catholic School north of Atlanta. She had taken Advair continuously for four years when, on an October night in 2011, she couldn’t breathe and was rushed to the hospital.
Brennan died in less than an hour, her parents said. An autopsy showed that her airways were filled with mucus. She was 11 years old.
Like the Wades a decade earlier, the Passonses scoured FDA material and talked to health-care professionals to find an explanation. They also looked at the Justice Department case.
Sarah Passons came to believe that Advair contributed to Brennan’s death — and that the FDA, Glaxo and the medical community had failed to adequately communicate the drug’s true risks.
Now, the family is encouraging pharmacies to do more to alert patients about the medication risks listed in drug package inserts. Advair’s insert, including a medication guide for patients, is more than 60 pages long.
Inserts can go unread, as the patient representative at the FDA’s 2008 advisory meeting acknowledged.
“I have to tell you,” said Andrea Holka, a Nebraskan with two asthmatic sons, “we’ve been taking different medications for the last 10 years for asthma, and I have yet to actually, embarrassedly, sit down and read an entire patient insert.”
Said Sarah: “I don’t want to see another child die.”
Editor’s note: The Sandler Foundation, the largest donor to ProPublica, also contributes to research into asthma, primarily through the American Asthma Foundation and the Sandler Asthma Basic Research Center at the University of California, San Francisco.
More stories like this: See Jeff Gerth’s reporting on Tylenol and its narrow margin of safety.
ProPublica is a Pulitzer Prize-winning investigative newsroom. Sign up for their newsletter.