The Alaska Native Medical Center in Anchorage, Alaska on Dec. 30, 2021. (Lyndsey Brollini/KTOO)
Respiratory viruses have been threatening hospital capacity in Alaska this winter. Dr. Matt Hirschfeld, a pediatrician with Alaska Native Medical Center in Anchorage, said flu and RSV cases started spiking early this year, in October.
“Usually, we don’t see these things start to peak until kind of December, January, February,” Hirschfeld said. “And then it’s also an extremely steep graph, meaning that a lot of people are getting infected all at once.”
At the same time, other viruses like parainfluenza, metapneumovirus and common colds are circulating too.
“It’s kind of a big soup of viruses that are happening out there,” he said.
Hirschfeld said this year’s cold and flu season has been worse, in part because COVID precautions were keeping people separated and keeping viruses at bay the last few years.
Most people get RSV, or respiratory syncytial virus, as children, but that doesn’t mean you can’t get it again as an adult. RSV and flu both have the strongest impacts on young children and elderly people.
Dr. Matt Hirschfeld in front of the Alaska Native Medical Center in Anchorage on Oct. 7, 2021. (Jeff Chen/Alaska Public Media)
State epidemiologist Dr. Joe McLaughlin said RSV usually causes mild, cold-like symptoms.
“Most people recover within a week or two, but it can cause serious illness especially for infants and older adults,” he said.
Serious cases typically present with wheezing or difficulty breathing, due to inflammation of small airways in the lungs.
Late last week Hirschfeld said pediatric hospital capacity in Anchorage was close to its limits.
“ANMC had a couple of beds, Providence was totally full. And most of the other hospitals had one or two beds or they were completely full,” he said.
Hirschfeld added that the majority of his patients live in rural Alaska and were transferred into the city for more specialized care.
Meanwhile, a nationwide shortage of amoxicillin, a type of antibiotic drug, is also affecting Alaska. State pharmacist Coleman Cutchins said the shortage is being driven by increased demand for the drug, not a manufacturing issue.
Amoxicillin shouldn’t be used to treat viral illnesses, but it can be prescribed for bacterial pneumonia and some ear infections, which tend to surge around cold and flu season.
Cutchins said it’s possible the amoxicillin shortage is in part due to it being overprescribed for patients who don’t need it.
“I haven’t heard of it not being available for people that totally need it. And there are alternatives,” Cutchins said. “But as we think about things in short supply, it’d be better to prevent yourself from being sick, to prevent the burden and the need for this type of drugs.”
RSV has already peaked on the East Coast, and epidemiologists are predicting Alaska is close to plateauing as well. But in the meantime, health officials are urging Alaskans to get flu shots and COVID boosters, practice regular hand-washing and stay home from gatherings if any symptoms arise.
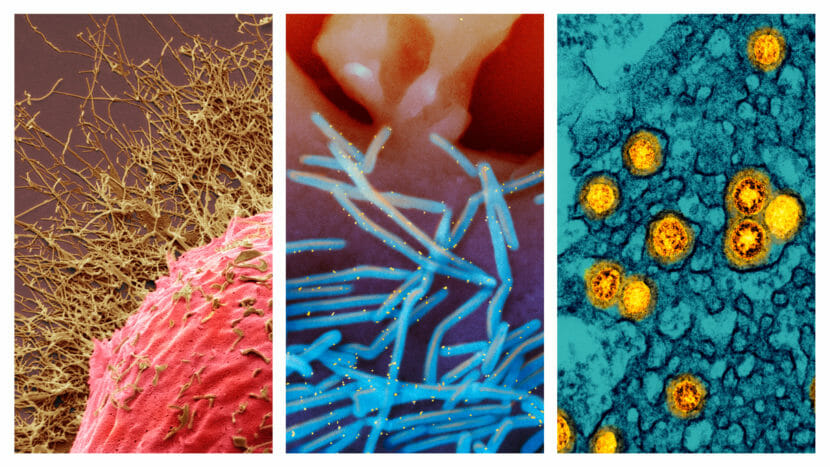
From left: 1) Colored scanning electron micrograph (SEM) of a human cell infected with H3N2 flu virus (gold filamentous particles). 2) Scanning electron micrograph of human respiratory syncytial virus (RSV) virions (colorized blue) that are shedding from the surface of human lung epithelial cells. 3) Transmission electron micrograph of SARS-CoV-2 Omicron virus particles (gold). (Science Source/ NIAID)
For each of the last two years, Thanksgiving helped usher in some very unwelcome guests: Devastating waves of COVID-19.
No one thinks this year will be anything like the last two dark pandemic winters, at least when it comes to COVID-19. But the country is now dealing with a different kind of threat — an unpredictable confluence of old and new respiratory pathogens.
“We’re facing an onslaught of three viruses — COVID, RSV and influenza. All simultaneously,” says Dr. William Schaffner, an infectious disease specialist at Vanderbilt University. “We’re calling this a tripledemic.”
Flu and RSV are back, big time
The respiratory syncytial virus (RSV) began surging unseasonably early this year, infecting babies and young children who had little or no immunity to that virus, which wasn’t circulating all that much over the past two years, in part, because of COVID-19 precautions.
“Intensive care units are at or above capacity in every children’s hospital in the United States right now,” says Amy Knight, president of the Children’s Hospital Association. “It’s very, very scary for parents.”
At the same time, an unusually early and severe flu season is surging, dominated by the H3N2 strain, which often strikes kids and older people especially hard.
“Influenza has hit the southeastern United States. It’s moved into the Southwest. It’s going up the East Coast and into the Midwest with some ferocity,” Schaffner says.
“Flu activity is high right now and continuing to increase,” says Lynnette Brammer, an epidemiologist in the CDC’s influenza division. “The good news is, the vaccines this year are well–matched to the viruses that are currently circulating, and there is still time to get vaccinated.”
But now comes another Thanksgiving.
“These holiday celebrations with all their travel and their close contact usually function as virus accelerators,” Schaffner says. “We’re spending a lot of time with each other. We’re laughing and breathing deeply. And that’s an ideal environment for these respiratory viruses to spread to others.”
What will COVID do this time?
Of course, COVID-19 is still sickening tens of thousands and killing hundreds of people every day. And new, even more contagious omicron subvariants that are especially adept at infecting people — even if they’ve been vaccinated or previously infected — are taking over.
“There’s a lot of moving parts here,” says Dr. David Rubin, who’s been tracking the pandemic at the PolicyLab at the Children’s Hospital of Philadelphia.
“What is this all going to mean for COVID? Are we going to see a January/February resurgence of COVID that’s going to be fairly significant? That may yet be coming.”
Many infectious disease specialists say the immunity people have from vaccinations and infections should keep any new surge of COVID-19 infections from causing a big increase in hospitalizations and deaths.
“I’m hopeful, given where we are with COVID, that we’re not looking at something like last winter. But at the end of the day, Mother Nature gets the final word on these things,” Dr. Ashish Jha, the White House COVID-19 Coordinator, told NPR.
“We’re in new territory here” with three viruses all circulating at high levels simultaneously, he says.
“I think it’s a really worrisome situation looking to the weeks coming ahead,” says Jennifer Nuzzo, an epidemiologist who runs the Pandemic Center at Brown University.
Nuzzo’s worried because an exhausted nation has abandoned many of the precautions people were taking to protect themselves and others. Flu vaccination rates are down by about 10% to 15% from previous years. Only about 11% of those eligible for the new bivalent omicron boosters have gotten boosted.
“We can’t just resign ourselves to assuming that it’s going to happen no matter what,” she says. “We can very much take action to prevent a rise in hospitalizations and deaths.”
Nuzzo and others experts say Americans can get vaccinated and boosted, especially if they are at high risk because of their age or other health problems.
People should consider Zooming for Thanksgiving if they’re sick, testing for COVID-19 before gatherings (especially those involving older friends and relatives and other vulnerable people), and even consider putting that mask back on as much as possible.
“If you’re not eating or drinking it’s probably a smart idea to protect the immunocompromised, the infants, as well as the older individuals in the household,” says Dr. Tina Tan, an infectious disease specialist at the Northwestern University Feinberg School of Medicine.
There are hints that RSV may already be peaking, and the flu could also peak early, before any new COVID-19 surge emerges. That would help relieve at least some of the pressure on hospitals.
There’s even a theoretical possibility that the flu and RSV could blunt any new COVID-19 surge in the same way the coronavirus crowded out those viruses the last two years. One possibility is a phenomenon known as “viral interference,” which involves the presence of one virus reducing the risk of catching another.
“COVID could be outcompeted, which is potentially good news,” Rubin says.
Copyright 2022 NPR. To see more, visit https://www.npr.org.
Transcript:
MARY LOUISE KELLY, HOST: To virus news now, specifically the fact that three viruses instead of just one are looming over this holiday season. NPR health correspondent Rob Stein brings us this update on the prospects for a so-called tripledemic.
ROB STEIN, BYLINE: For two years, Thanksgiving ushered in very unwelcome guests – devastating waves of COVID. No one thinks this year will be anything like those dark pandemic winters. But the country is facing something entirely new – an unpredictable mashup of old and new respiratory pathogens.
WILLIAM SCHAFFNER: We’re facing an onslaught of three viruses – COVID, RSV and influenza – all simultaneously.
STEIN: Dr. William Schaffner is an infectious disease expert at Vanderbilt University.
SCHAFFNER: We’re calling this a tripledemic.
STEIN: RSV crept back first, infecting lockdown babies and their older brothers and sisters with little immunity, overwhelming pediatric emergency rooms and intensive care units from coast to coast. The first big flu season in three years started early, too, sickening more kids with a strain that looks like it could be bad for their grandparents, too. That’s swamping more already understaffed, pandemic-spent hospitals. Here’s Lynnette Brammer from the CDC.
LYNNETTE BRAMMER: Flu hospitalization rates right now are the highest we’ve seen for this time of year in the past decade.
STEIN: And now Thanksgiving is coming. Dr. William Schaffner, again, from Vanderbilt.
SCHAFFNER: These holiday celebrations with all their travel and their close contact, usually function as virus accelerators. We’re spending a lot of time with each other, laughing and breathing deeply. And that’s an ideal environment for these respiratory viruses to spread to others.
STEIN: And, of course, there’s COVID still sickening tens of thousands and killing hundreds every day as new omicron subvariants are taking over that are even better at getting people, even if they’ve been vaxxed, boosted or previously infected.
DAVID RUBIN: The real question that we have is what is this all going to mean for COVID?
STEIN: Dr. David Rubin has been tracking COVID at the PolicyLab in Philadelphia.
RUBIN: We’re going to see a January, February resurgence of COVID that’s going to be fairly significant. That may yet still be coming.
STEIN: Immunity from all the COVID vaccinations and infections should blunt a new surge of serious illness, especially, Dr. Ashish Jha at the White House says, if people get one of the new bivalent omicron boosters.
ASHISH JHA: I’m hopeful, given where we are, that we’re not looking at something like last winter. But, look, at the end of the day, Mother Nature gets the final word on these things.
STEIN: And the new boosters aren’t finding a lot of takers; same for flu shots.
JENNIFER NUZZO: Yeah, I think it’s a really worrisome situation looking to the weeks coming ahead.
STEIN: Jennifer Nuzzo at Brown University’s Pandemic Center knows how done everyone is going into a third pandemic winter.
NUZZO: We can’t just resign ourselves to assuming that it’s going to happen no matter what. We can very much take action to prevent a rise in hospitalizations and deaths.
STEIN: Like – sorry – Zooming for Thanksgiving if you’re sick, doing one of those rapid tests the morning before hugging Grandma and Grandpa and, says Dr. Tina Tan from Northwestern, keeping that mask handy.
TINA TAN: If you’re not eating or drinking, it’s probably a smart idea to protect the immunocompromised, the infants, as well as the older individuals in the household.
STEIN: Now, here’s the good news. RSV may already be peaking, and the flu could peak early too, before colliding with a new COVID surge. There’s even a theory RSV and the flu could help stifle COVID like COVID crowded out those viruses the last two years. Fingers crossed for one of those scenarios to be thankful for this year. Rob Stein, NPR News. Transcript provided by NPR, Copyright NPR.
Antonio Rapuano got an infusion of a monoclonal antibody to treat his COVID in Albano, Italy in 2021. Such infusions have been effective treatments for COVID during the pandemic, but doctors are now finding that most monoclonal antibodies no longer work against new variants of SARS-CoV-2. (Photo by Yara Nardi/Reuters)
Monoclonal antibodies were once the star of COVID-19 outpatient treatments. Since they first became available in 2020 — even before the first vaccines — more than 3.5 million infusions of the factory-grown proteins have been given to patients in the U.S. to help reduce risk of hospitalization.
But one by one, different monoclonal treatments have lost their efficacy against new variants of the coronavirus. The rise of Paxlovid antiviral pills earlier this year, further dented their appeal.
Now, a new wave of omicron subvariants that are the best yet at evading the immune system’s current defenses have taken over in the U.S. They’re expected to knock out bebtelovimab, the last monoclonal antibody treatment standing against the coronavirus. Soon, it’ll join bamlanivimab, casirivimab, sotrovimab and others in the graveyard of monoclonals that once targeted past COVID strains until they were outflanked by variants that evaded their protection.
“Monoclonals had their day, like the Model T or the biplane,” says Carl Dieffenbach, director of the Division of AIDS at the National Institutes of Health, and lead of the NIH’s Antiviral Program for Pandemics, “Now it’s time to move on.”
Not everyone entirely agrees. Monoclonals are still useful, some doctors say, for treating a vulnerable population.
“There are severely immunosuppressed patients that are not likely to mount an immune response to the virus, even if you treat them with antiviral drugs,” says Dr. Raymund Razonable, an infectious disease specialist in the transplant division at the Mayo Clinic. “This is the group that is going to be the most affected by the absence of antibody-based therapies.”
What’s more new research is underway to develop new types of monoclonal antibodies that could even hold up against new variants.
How monoclonals work — and what they’re up against
Monoclonal antibody treatments have always had a major weakness – they’re easily outmaneuvered by new COVID strains. It’s a flaw that’s baked into how they work.
Monoclonal antibodies are lab-grown proteins that supplement your body’s immune system – which, in most people, is naturally producing antibodies to hunt for possible threats all the time.
“You and I and every human being that has a functioning immune system is walking around with probably trillions of totally different antibody molecules just circulating in our blood,” says Derek Lowe, a chemist and blogger for the journal Science, “Every one of us has a totally different suite of them. There are more of them than there are stars in the sky.”
The tiny, Y-shaped proteins lurk in the blood in low concentrations, “waiting and waiting until they happen to bump into something that they stick to really well, and they find their soulmate, basically,” Lowe explains. That “soulmate” is an antigen – a foreign substance that’s entered the bloodstream, like a bacterial protein or a virus or a pollen grain.
Once a monoclonal antibody finds its soulmate — in the case of COVID, a specific part at the tip of the SARS-CoV-2 virus – it binds to the surface of the antigen. Then, it sends out signals to the immune system, “like hey, I’ve got a live one,” Lowe says.
The most powerful antibodies can stop the virus in its tracks just by binding to it. For instance, “if you have an antibody that sticks to the tip of the spike protein at the business end of the virus – just the fact that it is stuck tightly to that means the virus cannot infect a cell,” says Lowe.
The spike protein has been the target of all the monoclonal antibody treatments that go after the virus thus far. But it’s been a fickle soulmate, changing with new variants, leaving the monoclonal antibodies adrift in the bloodstream with nowhere to bind.
Companies have stopped bringing these monoclonals to market. The federal government stopped promising to buy them in quantity, making it a riskier bet for companies.
“There are antibodies out there, but nobody has the $200 million to develop it,” Dieffenbach says, citing costs that include producing the antibodies, running trials and getting them authorized by the Food and Drug Administration. Some companies figured it wasn’t worth it, for a product that was likely to become obsolete in a matter of months, he says.
To be clear, these are antibody treatments for outpatient treatment. There is a different kind of monoclonal antibody treatment for hospitalized patients that remains viable. Actemra, as it’s called, is not susceptible to virus mutation because it targets the body’s immune reaction to the virus, rather than the virus itself.
New directions in research, and a potential comeback
There might still be hope for monoclonals. Drugmakers and researchers at government agencies are now retooling the strategy, looking for monoclonal antibodies that could last.
“Initially, the focus was, ‘let’s just find the most potent antibodies,'” says Joshua Tan, chief of the Antibody Biology Unit at NIH. “Now, there’s awareness that we need to find antibodies that are likely to work against not just the [current version of the] coronavirus, but whatever may come.”
In his lab in Rockville, Md., Tan and the researchers who work with him are looking for antibodies that target parts of the virus that have stayed the same on several different viruses within the larger coronavirus family. “We’re looking at other parts of the spike protein that may be more consistent and may be harder to mutate,” Tan says.
To achieve this, researchers in Tan’s lab are taking immune cells from the blood of patients that have recovered from COVID, and pelting them with tiny plastic pellets covered with spike proteins from different, older coronaviruses to see which cells respond. “Not the [COVID] variants, but SARS-CoV-1, SARS-CoV-2, MERS [etc.],” post-doctoral researcher Cherrelle Dacon clarifies. “These are seven different coronaviruses, all of which infect humans.”
The immune cells that react to several different coronaviruses are making antibodies that bind to a part of the spike protein that’s staying the same across them.
It’s a painstaking process: Isolating individual immune cells, finding the ones that make antibodies in response to various spike proteins — and then using those to make more antibodies that they can scale up, analyze and test, to figure out what on the virus they’re actually binding to. The process takes about three to four months each cycle, Tan says.
Tan says the good news is that they’ve found some antibodies that stick to multiple different coronaviruses. They published some of the results earlier this summer in Science.
But the problem the researchers have come up against is that the monoclonal antibodies they’ve found are not so potent. Tan says there seems to be a tradeoff – between how well a monoclonal antibody against COVID-19 works, and how long it lasts before the virus ditches the antibody’s target.
An analogy: If the coronavirus had human body parts (which it doesn’t) the old, highly effective monoclonals hit the virus’s spike protein squarely on the nose. In contrast, the new monoclonals Tan is finding try to grab it by the armpit. “One of the issues appears to be that it’s harder to reach those parts,” Tan says, “What the broader, less potent [antibodies] need is for the spike protein to shift in shape” in order for them to grab it.
Tan is working to find ways around this tradeoff. He says you can potentially modify the antibody, change out parts of it to increase its potency – a process that’s largely theoretical at the moment, and will take some time to work out.
So while Tan and other researchers work on the next generation of monoclonal antibodies – ones that work well against all kinds of coronaviruses, maybe even future pandemic ones – the nation is entering a long lull with no monoclonal antibody treatments that work against dominant strains of SARS-CoV-2.
“The disappointment is there because you’re losing a really good drug,” says Razonable. “But you focus on the next options. The virus adapts, and we also adapt based on what we have available.”
Luckily, as Tan and others pursue the long game with antibodies, there are other treatments, like Paxlovid pills and remdesivir infusions, that still work against COVID.
And the research on and rapid development of antibody treatments has opened up possibilities beyond COVID. “It has improved the production of monoclonals for cancer, for immunologic diseases,” says Dieffenbach, “It’s going to be easier to produce monoclonals in the future because of the lessons learned from SARS-CoV-2. Nothing was wasted here.”
Copyright 2022 NPR. To see more, visit https://www.npr.org.
Transcript:
RACHEL MARTIN, HOST:
As new COVID variants rise here in the U.S., antibodies are getting wiped off the list of treatments. NPR’s Pien Huang explains why these infusion treatments didn’t last and how scientists are searching for a new generation of antibodies that might.
PIEN HUANG, BYLINE: Over the pandemic, more than 3 million COVID patients have gotten infusions of antibodies to help keep them out of the hospital. Carl Dieffenbach, a top official with the National Institutes of Health, says that now with new immune-evasive COVID variants, these so-called monoclonal antibody treatments are out.
CARL DIEFFENBACH: Monoclonal antibodies had their day, like the Model T or like the biplane, and now it’s time to move on.
HUANG: The antibody treatments have always had a major weakness – they’re easily taken out by new COVID strains. And it’s a flaw that’s baked into how they work. Antibodies are tiny Y-shaped proteins that float around in your blood. Derek Lowe, a chemist and blogger for the journal Science, says they look for very specific targets.
DEREK LOWE: And they’re just circulating around, waiting and waiting until they happen to bump into something that they stick to really well, and they find their soulmate, basically.
HUANG: Once they stick to their soulmate – in this case the SARS-CoV-2 virus – they tell the immune system to send reinforcements. Lowe says the most powerful antibodies can stop the virus in its tracks.
LOWE: If you have an antibody that sticks to the tip of the spike protein at the business end of the virus, just the fact that it is stuck tightly to that means the virus cannot infect a cell.
HUANG: But the tip of the spike protein is a fickle soulmate. It changes as the virus mutates, leaving the antibodies adrift in the bloodstream with nowhere to bind. Companies have stopped bringing these antibody treatments to market because they cost millions of dollars to develop, and they’re obsolete in a matter of months. So researchers are changing gears to look for antibodies that could last. Joshua Tan is head of the Antibody Biology Unit at the NIH. He showed me around his lab in Rockville, Md.
JOSHUA TAN: This is going to orient the tour ’cause I’m going to walk you through the different steps that we have.
HUANG: He and the researchers that work with him are taking immune cells from the blood of patients that have recovered from COVID, and they’re pelting them with tiny plastic pellets covered with spike proteins from different coronaviruses. Cherrelle Dacon, a postdoctoral researcher at the lab, explains.
CHERRELLE DACON: And so the spike proteins coat the surface of the beads. This is, like, seven different coronaviruses. So SARS-CoV-1, CoV-2, MERS, HKU-1.
HUANG: The cells that react to several coronaviruses are reacting to a part of the spike protein that’s staying the same across them. Tan says the good news is that they have found some antibodies that stick to multiple coronaviruses, and they’ve published results in the journal Science. But the problem that they’re coming up against is that the ones that they found are not so potent. Tan says if the old antibodies hit the virus on the nose, the new ones that he’s finding kind of grab it in the armpit.
TAN: At least one of the issues appears to be that it’s harder to reach those parts. They need the spike protein to shift in shape.
HUANG: It’s a less direct attack, so there seems to be a trade-off between how well an antibody treatment works and how long it lasts. Tan’s looking for ways around this trade-off by tweaking parts of the antibody. Luckily, as Tan and others pursue the long game, there are other treatments, like Paxlovid and remdesivir, that do still work against COVID.
Pien Huang, NPR News. Transcript provided by NPR, Copyright NPR.
New COVID variants that are highly immune evasive have overtaken BA.5 to dominate in the U.S. Experts warn this means more reinfections and a possible winter surge. (Photo by Spencer Platt/Getty Images)
Two new omicron subvariants have become dominant in the United States, raising fears they could fuel yet another surge of COVID-19 infections, according to estimates released Friday by the Centers for Disease Control and Prevention.
The subvariants — called BQ.1 and BQ.1.1 — appear to be among the most adept yet at evading immunity from vaccination and previous infection, and have now overtaken the BA.5 omicron subvariant that has dominated in the U.S. since the summer.
“It’s a little bit eerily familiar,” says Dr. Jeremy Luban of the University of Massachusetts, who’s been tracking variants since the pandemic began.
“This time of year last year we were optimistic. We were coming out of the delta wave, and it was steadily decreasing, and we went into Thanksgiving to wake up to omicron. So there is this sort of déjà vu feeling from last year,” Luban says.
BQ.1 and BQ.1.1, had been quickly gaining ground in the U.S. in recent weeks. On Friday, they officially overtook BA.5, accounting for an estimated 44% of all new infections nationwide and nearly 60% in some parts of the country, such as New York and New Jersey, according to the CDC’s estimates. BA.5 now accounts for an estimated 30% of all new infections nationwide.
Recent laboratory studies indicate that new mutations in the virus’s spike protein appear to make BQ.1 and BQ.1.1 as much as seven times more “immune-evasive” than BA.5.
But even if the new subvariants do surge this winter, most experts think any uptick in infections won’t hit as hard as the first two winter surges of the pandemic.
“We are hoping that the amount of immunity that has been induced either by prior infection or by vaccination” will protect most people from getting severely ill or dying, Dr. Anthony Fauci, the White House medical advisor, told NPR.
That said, a new study suggests that getting reinfected with the virus still can pose significant risks, both for short term and long-term complications, including an increased risk of hospitalization, symptoms of long COVID and even death.
“The risk of reinfection is definitely not trivial,” says Ziyad Al-Aly, an assistant professor of medicine at Washington University School of Medicine in St. Louis and an author of the new study. “So going into the winter surge now people should do their best to try to prevent getting reinfected.”
“You’re basically playing Russian Roulette again,” he says. “You may dodge the bullet the next time around, but it may not be the case.”
Because the newly dominant variants appear to be highly immune-evasive, many people may get reinfected.
“The bad news is that it’s likely that people who’ve been vaccinated and/or infected will still get infected” with these new subvariants, says Dr. Daniel Barouch, a virologist at Beth Deaconess Hospital in Boston who’s been studying the new strains.
The new strains are becoming dominant just as winter is approaching and people will be traveling and gathering for the holidays, factors that had already raised fears about another winter surge.
“The U.S. is going to see a winter surge in COVID infections,” predicts William Hanage, an epidemiologist at the Harvard T.H. Chan School of Public Health. “And I think that if nothing else changes BQ.1 and BQ.1.1 are likely to be very significant players.”
The key question is the scale of any winter surge that does emerge.
“The question is whether this increase is going to be nationwide and whether the size of the increase and the surge will be something like what we experienced with delta and omicron, or much smaller,” says Samuel Scarpino, vice president of Pathogen Surveillance for the Rockefeller Foundation.
“I think it’s quite concerning,” he adds.
Infections, and even hospitalizations, have already started inching up in some parts of the country.
One promising sign is that recent surges in other countries suggest that if the subvariants are involved in a new U.S. wave, any uptick could be short-lived. For example, while France experienced a surge involving the new subvariants, the increase in cases quickly receded.
Nevertheless, experts are urging more people to get one of the updated boosters, which for the first time target omicron.
“Hopefully, more people will go and get their updated vaccine — the bivalent vaccine,” Fauci says. “That will mitigate a real surge and at worst we’ll get a blip versus a major surge.”
While some preliminary studies have questioned whether the new boosters are any better than the original vaccine at protecting against omicron, others have suggested they may be. Vaccine makers Pfizer and BioNTech recently released a statement saying their new booster stimulates much higher levels of antibodies that can neutralize the BA.5 omicron subvariant than the original vaccine.
Wade Marrs competing in the 2020 Iditarod. Marrs ran Iditarod again in 2021 but opted out in 2022 after 10 consecutive races, citing the Iditarod’s requirement for mushers to be vaccinated against COVID-19. (Photo by Zachariah Hughes/Alaska Public Media)
The Iditarod Trail Sled Dog Race is dropping its COVID-19 vaccination requirement for mushers, staff and volunteers in the 2023 race.
The announcement comes as mushers have been slow to sign up for the 51st running of Iditarod, with only 26 listed as of Tuesday. Past years have seen as many as 80 or 90 teams start the 1,000-mile race from Anchorage to Nome.
But Iditarod spokeswoman Shannon Noonan said having fewer mushers signed up did not affect the decision to drop the vaccination requirement.
“You know, dropping this policy may change that, but that was not a deciding factor of dropping the vaccination policy,” Noonan said.
Last year, the Iditarod said requiring proof of vaccination was necessary to protect everyone along the trail. That included residents of remote communities serving as checkpoints, where medical care is limited and an influx of people during the race could lead to an outbreak. The village of Takotna, a favorite stop for some mushers to take their mandatory 24-hour break, opted out of being a checkpoint altogether in 2022, out of concern for residents’ health.
What’s different now, Noonan said, is COVID’s declining trajectory in Alaska. State and federal guidelines aren’t recommending vaccination requirements for big events like the Iditarod.
“We in no way are dropping the vaccine requirement, you know, saying that COVID is over, in any way,” Noonan said. “We are, absolutely still have, our villages and our mushers and our volunteers as our number one concern, and we’re going to continue asking and looking for input from our villages as we move forward to the race.”
It’s unclear if dropping the vaccination requirement will bring back mushers who cited the policy when they decided not to race the Iditarod in 2022. That includes Wade Marrs, who had mushed the previous 10 races and placed 4th in 2021, matching his previous best finish, but said he wouldn’t race in 2022 because of the vaccination requirement.
Five-time Iditarod finisher Monica Zappa, of Kasilof, has been skeptical of the vaccines and opposed the Iditarod’s requirement. And while she said her decision not to race the past two years also involved the age of her dogs and the cost of maintaining a race kennel, Zappa said she’s glad the race is dropping the requirement.
“I mean, I’m not like begrudging the race, but sometimes just in life in general, you have to let people be the controllers of themselves a little bit, too,” Zappa said.
Noonan, with the Iditarod, said race officials are still discussing protocols for COVID-19 testing during the race. In 2021 and 2022, a positive test meant mushers or staff had to leave the race.
Meantime, Noonan said the Iditarod is hoping more mushers — some wrapping up their first busy tourism season since before the pandemic — will sign up for the 2023 race.
If the start were today, the 26 teams currently listed would be, by far, the fewest in Iditarod history. Mushers can still sign up, but the entry fee increases at the end of November.
Alaska Native Medical Center nurse Rocky Carloni rolls up her sleeve before getting a COVID-19 booster shot. (Photo by Nat Herz/Alaska Public Media)
State health officials are encouraging Alaskans to get their COVID-19 bivalent boosters as case numbers and hospitalizations increase in Europe.
At a public health presentation Wednesday, state epidemiologist Dr. Joe McLaughlin said an omicron wave in Germany is showing the importance of getting boosted.
“One of the challenges that Germany is facing is that they have really low vaccination coverage rates, especially with the booster,” he said. “That’s one of the things they’re attributing to the high rates of infection and hospitalization.”
Here in Alaska, McLaughlin said, COVID hospitalization numbers are decreasing. But hospital utilization — the percentage of hospital beds being used — has steadily increased in Alaska since the start of the pandemic. That could be due to a number of factors like staff shortages, he said, but it’s an important sign to watch as flu season begins.
Bivalent COVID boosters, which target both the original strain and its omicron variants, have been available to adults for more than a month. The CDC authorized the boosters for children as young as 5 last week.
State physician Dr. Lisa Rabinowitz said uptake for the new booster and the flu shot has been slow.
“The flu vaccine was a little delayed in shipping out nationally, so I think due to that we’ve had a little slower uptake,” she said. “But I’m excited to see some traction on this as we move into the fall.”
She said it’s safe to get the flu shot and the COVID booster at the same time. If you’ve had COVID recently, you’ll have adequate protection against the virus for about three months. But Rabinowitz said it’s also safe to get it as soon as your symptoms have gone away.
“Especially for those individuals that know they’re going to be traveling or around people that are at higher risk for COVID, maybe it makes sense to get vaccinated sooner than waiting that three months,” Rabinowitz said. “But either is a viable option.”
Alaskans can get boosted by visiting vaccines.gov, contacting their primary care provider or local public health clinic, or calling the state’s COVID helpline at 907-646-3322. You can also text your ZIP code to 438829 to find a nearby provider.
Close
Update notification options
Subscribe to notifications
Subscribe
Get notifications about news related to the topics you care about. You can unsubscribe anytime.



9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))

9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))

9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))

