Bartlett Regional Hospital, pictured here on Dec. 1, 2018, is located at 3260 Hospital Drive in Juneau. (Photo by Jeremy Hsieh/KTOO)
Bartlett Regional Hospital will close its COVID-19 monoclonal antibody therapy clinic on Oct. 24.
The clinic offered treatments to help prevent serious illness in newly infected, high risk COVID-19 patients. In a press release, the hospital cited a decrease in demand.
“For the entire month of September, we only had 8 appointments filled, and we offer around 48 appointments per month,” Bartlett’s community relations director Erin Hardin said. “We used to have regularly filled appointments.”
Bartlett will continue providing a drug called Evusheld, which helps prevent COVID-19 infections for immunocompromised individuals who are fully vaccinated or haven’t received a COVID-19 vaccine for medical reasons if they aren’t already infected with or recently exposed to the virus.
In mid-November, the hospital is also getting rid of its drive-through COVID testing site.
COVID-19 PCR testing continues to be available through SEARHC — free for symptomatic patients and $145 for asymptomatic patients — and Juneau Urgent Care, which is also free for symptomatic patients and $275 for asymptomatic patients.
Free at-home test kits are still available for free at City Hall, the Juneau Public Health Center, public libraries and the police station.
Correction: A previous version of this article misstated the purpose of Evusheld.
Alaska Chief Medical Officer Dr. Anne Zink discusses the state of the coronavirus pandemic during a news conference at the Atwood Building in Anchorage on Thursday, Aug. 26, 2021. (Matthew Faubion / Alaska Public Media)
The Alaska Department of Health and Social Services sent out its last COVID-19 data summary on Wednesday via email and social media. It marks a shift from focusing on case counts to tracking broader trends across the state.
The department will continue to send its weekly COVID and flu update on Fridays. Alaska’s chief medical officer, Dr. Anne Zink, said those updates will still include COVID case counts.
“But we try to put that into a larger context,” she said. “We also talk about how many people show up to the emergency department for COVID-like illness, how many people are showing up to the emergency department for influenza-like illness, and how full the hospitals are in general.”
Wednesday’s data summary reported 34 hospitalizations and 546 resident cases in the last week. Zink said it’s become harder to track case numbers as home tests have become more popular because those results don’t always get reported to the state.
“It’s become increasingly problematic as we have more home testing, and why we need to use it in combination with other data sources to give Alaskans the best sense that they can of the overall transmission of respiratory illnesses in their community at any given time,” Zink said.
Zink said there are important differences between COVID and the flu to keep in mind when it comes to risk level. Older Alaskans are still at the highest risk for severe illness and death due to COVID, while flu carries increased risk for both the very young and the very old.
“People should consider getting flu vaccines now, anyone six months and older, particularly the young and the old,” she said. “Or, honestly, people who interact with the young or the old, which is a lot of us.”
The bivalent COVID booster — which teaches the immune system to fight both the original COVID strain and the omicron variant – has been available for about two weeks. It’s safe to get the booster and the flu vaccine at the same time.
According to state data, 28% of all Alaskans aged 6 months and older have received a first booster dose. In Juneau, 44% of residents 6 months and older have received a first booster, and 31% of Anchorage residents have. The lowest percentage is in the Matanuska-Susitna Borough, at nearly 17%.
Zink said many hospitals and long-term care facilities are administering COVID boosters and flu vaccines at the same time, and she expects booster numbers to increase as those efforts continue.
Zink recommends getting a flu shot by the end of October. And as fall turns to winter, she said, taking care of your mental and physical health is extra important.
Stevi Frets and Max Pyles joke as they do the dishes at the Sun’aq Tribe’s language house in Kodiak on Sept. 15, 2022. (Photo by Claire Stremple/KTOO)
Half of the first language speakers of Kodiak Alutiiq died between 2020 and 2022. But that’s not stopping new speakers from learning the language and passing along a distinct culture and worldview to the next generations.
At the Sun’aq Tribe’s language house, everything is a lesson—catching up on gossip, making a grocery list or washing the dishes.
No one lives here full time, but the Sun’aq Tribe uses a federal grant to pay a group of language apprentices and mentors to master the language.
“To really get the language down, you gotta use it in practice,” said Dehrich Chya, a mentor at the language house. “The point of a language house is it’s a place where you can just get together and use the language in your day to day life.”
“Heritage languages are so important,” said mentor Stevi Frets. “And when you learn them, it’s like, ‘Okay, I’m part of the crew saving it now.’ There’s no like, ‘Yeah, I learn a little Alutiiq on weekends, when I can.’ All of a sudden, you’re like, ‘Oh, my gosh, my language, I have to save it, I have to do everything I can’.”
Kodiak is home to a powerful movement to bring the Alutiiq language back into daily use. For about 100 years, American schools and governments suppressed the language and punished children for speaking it. Now the last Elders who speak it fluently are almost gone.
Frets says there are a few Elders in town she can speak with, and a lot of folks who have gone through some basic language classes at the University.
“But there’s not a lot of people you can like have a conversation with around. Like, I think they’re mostly in this room right now,” she said with a laugh.
In some ways, Frets says she feels like she missed out. The tribe estimates there are now only about 17 Elders who are fluent Alutiiq speakers left. They lost about that many during the pandemic. It’s a turning point.
But the language movement isn’t giving up, it’s moving forward.
Hailey Thompson administers the grant. She says part of the Sun’aq Tribe’s goal is to train fluent speakers who can in turn teach the language.
“We have a lot of motivation to learn Alutiiq. People want Alutiiq preschools, and Alutiiq language classes at the high school, and Alutiiq language class at the college,” she said. “But the problem is we don’t have the teachers to teach those classes and workshops.”
Hailey Thompson manages the Sun’aq Tribe’s language grant. “It’s not a job you can just clock out of,” she said. “If we don’t build more Alutiiq fluent people… then there’s not going to be anyone for my kids to learn from. So that’s what probably keeps me going.” In Kodiak on Sept. 15, 2022. (Photo by Claire Stremple/KTOO)
A solid foundation of language revitalization already exists in Kodiak. But Thompson says it’s different now—there were a lot more elders before.
“The next wave of what it looks like is building resources, archiving things that we know we’re going to need, spending the time that we know we can get with elders,” she said. “That’s what it looks like right now. Just cherishing all the things, that all the resources we can get… before we know that they’re gone.”
The stakes are high, but the rewards are immense. Frets and the others are building fluency to be able to teach the next generation of Alutiiq speakers.
At the Alutiingcut Childcare Center about a dozen preschoolers learn numbers in Alutiiq and Alutiiq versions of popular kids songs. There probably won’t be any birth speakers left by the time they’re older, but the language movement is working to ensure they’ll have teachers.
An Alutiiq language program exists at the Kodiak college and courses at the high school. And the tribe hopes to put 18 people through its program at the Language House over the course of its 3-year grant.
Learners meet up with Elders at the museum once a week. Three of the Elders that used to be at those sessions died during the pandemic, but the museum records them so new learners and descendants of the speakers can hear their stories.
Dehrich Chya, the Alutiiq Museum’s Language and Living Culture director, sits with Elders at a weekly session in Kodiak on Sept. 16, 2022. (Photo by Valerie Kern/AKPM)
Florence Pestrikoff didn’t grow up speaking Alutiiq, even though most people in her village did. But for the last couple of decades she has been an active speaker and teacher–she learned in the first wave of language revitalization about 20 years ago.
“I love speaking my language,” she said. “In the past it was — people were ashamed of the language. It’s sad. Really sad.”
American missionaries and schools enforced strict English-only policies for years. Parents like hers encouraged English to protect their children. The result was a swift decline in speaker numbers.
Pestrikoff answers her cell phone in Alutiiq and says she speaks it with her husband. And that’s the vision of the language movement—to have the language be in use. At home, in the grocery store, on the street.
And to carry the values that are embedded in the words.
“We never say goodbye. There is no goodbye in Alutiiq,” Pestrikoff said. “You say ‘Tang’rciqamken. I will see you later.’ I like that.”
Just like the language in Kodiak schools and homes — quiet for a while, but coming back.
Luke Dihle, RN at Bartlett Hospital, leaves a triage tent near the entrance of the hospital on Monday, April 7, 2020 in Juneau, Alaska. (Photo by Rashah McChesney/KTOO)
How public health systems collect and report data during a pandemic can help determine how diseases spread and how to stop them. But a New York Times investigation shows that data in Alaska — and across the nation — continues to be lost or unusable due to under-investment in public health.
Reporter Sharon LaFraniere traveled to Alaska for the story. She says Alaska’s data shortfalls during the pandemic weren’t unusual — and the only solution is spending money to modernize public health systems.
Listen:
The following interview has been edited for length and clarity.
Claire Stremple: What’s the data failure? How did it happen?
Sharon LaFraniere: The government never invested enough money to modernize the data systems for state and local governments. Over the past decade, we spent $38 billion to modernize health records at hospitals and clinician’s offices. And we’re seeing results from that now, like if you go into your doctor’s office, and many places, the doctor can right there, you know, look up your electronic record. But we didn’t spend the same. We didn’t spend money to modernize the state and local health departments. We left them with the spreadsheets, telephones, fax machines, Excel sheets. The old system. I think many people don’t understand–and I certainly didn’t understand, until I got into this–how behind state and local health departments are in the data. They’re way behind.
Claire Stremple: You wrote that the low vaccine rate contributed to the heavy death toll in the United States from COVID-19. But so did the lack of data. Why is that deadly?
Sharon LaFraniere: Nobody can pinpoint we lost XX million, or how many other people became severely ill from COVID, because we didn’t have data. But basically what happened is the fact that the data pipeline, if you think of the digital pipeline, is totally riddled with holes and obstacles, and it doesn’t flow. It means that the government did not respond as quickly as it could have. Because to some degree, they were flying a little bit blind. All the senior federal health officials that I’ve spoken to in the last three years are utterly convinced it had a real impact.
Claire Stremple: What made you come to Alaska to tell this story?
Sharon LaFraniere: Two reasons. One, the Alaska State Health Department is a pretty hard charging health department, and it has a lot of talented people in it.
Secondly, because its problems are quite typical.
Claire Stremple: What was the atmosphere like when you were here. What did you see? Did anything kind of stand out to you while you were reporting?
Sharon LaFraniere: I mean, I’m saying this not to be flattering, but I think the health department is incredibly hard working and very dedicated. I mean, why else would you be carrying stacks of paper, you know, from the fax machine at 6 a.m. and entering it all by hand if you didn’t really care?
Claire Stremple: You reported a lack of race and ethnicity data. How does that happen? And what are the consequences?
Sharon LaFraniere: So race and ethnicity is one of the data fields that is often just left out. And so for instance, in Alaska, the someone has a COVID test and they test positive, the lab test comes back in 6out of 10 cases where the field that says race and ethnicity is simply left blank. And so the health authorities don’t want to say, ‘hey, we’re not going to process these results, because you left this critical information blank.” They process the results. But then when Dr. Zink wanted to know about the disparate rate of COVID testing among minorities–she basically was trying to figure out where Alaska needed to put more testing sites to correct this–and she couldn’t get an answer because that field was left blank way too often. It matters when you’re trying to figure out how to allocate resources.
Claire Stremple: What are the consequences of using trained epidemiology staff to do a bunch of manual data entry? You know, what could they have been doing instead? And what did epi staff in Alaska have to say about this?
Sharon LaFraniere: To me was one of the more troubling things is that if you, I mean, think of it like if your phone didn’t sync with your computer, right? Then you enter your information in the phone, you’re going to enter it again in the computer. That’s what was happening here. So a whole bunch of people had to be roped in to re-enter information because the databases could not connect with each other. So the health department was forced to basically reduce some of its most highly trained epidemiologists, for periods of time, simply to enter data.Cecause the data had to be entered. So they would do it on weekends, they would do it at night. So it would start at 6am. It was an immense amount of effort, just to get the data entered. And that’s not unusual. And then a disturbing thing about it is people put in all that effort, and then a lot of it wasn’t useful. Because the date by the time the data got entered, it was too late to be meaningful, or it was too incomplete to guide decision making.
Claire Stremple: In your reporting did you or did anyone you spoke to have a sense of how we fix it?
Sharon LaFraniere: I mean, you fix it by money. Basically, if the system is upgraded, then there are faster ways to fill in the missing information, right? And it’s not just money, it’s not just that they need software and better systems and all that–they need the people to run the systems, right? They need data scientists and data analysts and people who are trained as an epidemiologist and as data scientists, and they don’t have those people, they have a completely skeletal staff.
Claire Stremple: To your point about money, Alaska got less funding than expected, much less funding than expected for improvements. What are the consequences of that? And why is it still not a priority?
Sharon LaFraniere: I’m not sure why Alaska didn’t get more money, like why its share of the pot was less. But I know that the pot is too small. And when you divvied up among fifty states, what Alaska ended up with from this latest grant, a five year grant was about $1.8 million a year for that for public health personnel and infrastructure. And of that there was $213,000 a year for data modernization. And, like one of the state health officials said, ‘Well, that’s about enough for a nice campervan.’ It’s partly that I think Congress allotted a certain amount of money, but it just isn’t enough money.
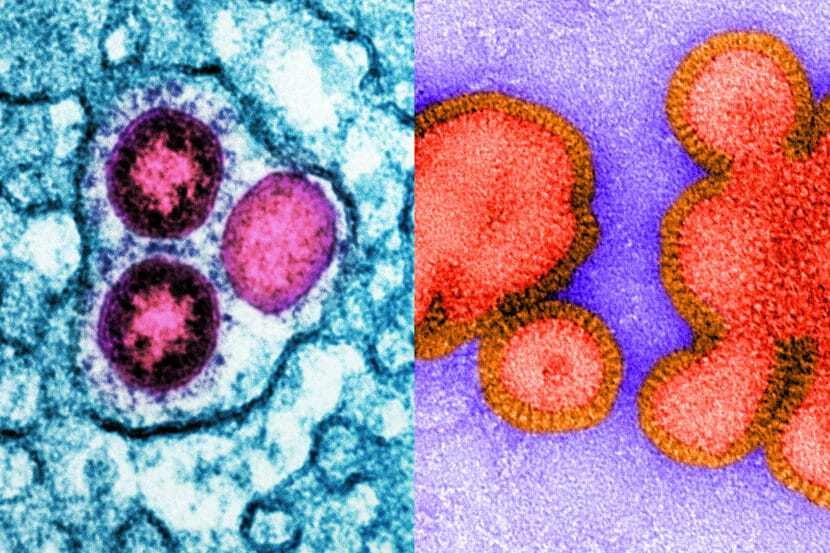
Health officials are predicting this winter could see an active flu season on top of potential COVID surges. In short, it’s a good year to be a respiratory virus. Left: Image of SARS-CoV-2 omicron virus particles (pink) replicating within an infected cell (teal). Right: Image of an inactive H3N2 influenza virus. (NIAID/Science Source)
The flu virtually disappeared for two years as the pandemic raged. But influenza appears poised to stage a comeback this year in the U.S., threatening to cause a long-feared “twindemic.”
While the flu and the coronavirus are both notoriously unpredictable, there’s a good chance COVID cases will surge again this winter, and troubling signs that the flu could return too.
“This could very well be the year in which we see a twindemic,” says Dr. William Schaffner, an infectious disease professor at Vanderbilt University. “That is, we have a surge in COVID and simultaneously an increase in influenza. We could have them both affecting our population at the same time.”
The strongest indication that the flu could hit the U.S. this winter is what happened during the Southern Hemisphere’s winter. Flu returned to some countries, such as Australia, where the respiratory infection started ramping up months earlier than normal, and caused one of the worst flu seasons in recent years.
What happens in the Southern Hemisphere’s winter often foreshadows what’s going to happen north of the equator.
“If we have a serious influenza season, and if the omicron variants continue to cause principally mild disease, this coming winter could be a much worse flu season than COVID,” Schaffner warns.
And the combination of the two viruses could seriously strain the health system, he says. The Centers for Disease Control and Prevention estimates that flu causes between 140,00 and 710,000 hospitalizations annually.
“We should be worried,” says Dr. Richard Webby, an infectious disease specialist at St. Jude Children’s Research Hospital. “I don’t necessarily think it’s run-for-the-hills worried. But we need to be worried.”
The main reason the flu basically disappeared the last two years was the behavior changes people made to avoid COVID, such as staying home, avoiding public gatherings, wearing masks, and not traveling. That prevented flu viruses from spreading too. But those measures have mostly been abandoned.
“As the community mitigation measures start to roll off around the world and people return to their normal activities, flu has started to circulate around the world,” says Dr. Alicia Fry, who leads influenza epidemiology and prevention for the CDC. “We can expect a flu season this year — for sure.”
Young kids at especially high risk
The CDC is reporting that the flu is already starting to spread in parts of the south, such as Texas. And experts caution very young kids may be especially at risk this year.
Though COVID-19 generally has been mild for young people, the flu typically poses the biggest threat to both the elderly and children. The main strain of flu that’s currently circulating, H3N2, tends to hit the elderly hard. But health experts are also worried about young children who have not been exposed to flu for two years.
“You have the 1-year-olds, the 2-year-olds, and the 3-year-olds who will all be seeing it for the first time, and none of them have any preexisting immunity to influenza,” says Dr. Helen Chu, assistant professor of medicine and allergy and infectious diseases and an adjunct assistant professor of epidemiology at the University of Washington.
In fact, the flu does appear to have hit younger people especially hard in Australia.
“We know that schools are really the places where influenza spreads. They’re really considered the drivers of transmission,” Chu says. “They’ll be the spreaders. They will then take it home to the parents. The parents will then take it to the workplace. They’ll take it to the grandparents who are in assisted living, nursing home. And then those populations will then get quite sick with the flu.”
“I think we’re heading into a bad flu season,” Chu says.
‘Viral interference’ could offset the risks
Some experts doubt COVID and flu will hit the country simultaneously because of a phenomenon known as “viral interference,” which occurs when infection with one virus reduces the risk of catching another. That’s an additional possible reason why flu disappeared the last two years.
“These two viruses may still both occur during the same season, but my gut feeling is they’re going to happen sequentially rather than both at the same time,” Webby says. “So I’m less concerned about the twindemic.”
Nevertheless, Webby and others are urging people to make sure everyone in the family gets a flu shot as soon as possible, especially if the flu season arrives early in the U.S. too. (Most years officials don’t start pushing people to get their flu shots until October.)
So far it looks like this year’s flu vaccines are a good match with the circulating strains and so should provide effective protection.
But health officials fear fewer people will get flu shots this year than usual because of anti-vaccine sentiment that increased in reaction to COVID vaccinations. Flu vaccine rates are already lagging.
“We are worried that people will not get vaccinated. And influenza vaccine is the best prevention tool that we have,” the CDC’s Fry says.
Fry also hopes that some of the habits people developed to fight COVID will continue and help blunt the impact of the flu.
“The wild card here is we don’t know how many mitigation practices people will use,” Fry says. “For example, people now stay home when they’re sick instead of going to work. They keep their kids out of school. Schools are strict about not letting kids come to school if their sick. All of these types of things could reduce transmission.”
Copyright 2022 NPR. To see more, visit https://www.npr.org.
Transcript:
STEVE INSKEEP, HOST:
For the last two years, the flu mostly disappeared. People who isolated to duck COVID also avoided influenza. Did you notice this? Hardly anybody in my family got sick with anything for a while. But what happens this year as so many people are back at work and school unmasked? NPR health correspondent Rob Stein joins us now. Good morning.
ROB STEIN, BYLINE: Good morning, Steve.
INSKEEP: How serious could this year’s flu season be?
STEIN: You know, Steve, the first thing I should say is that the flu is notoriously unpredictable, so it’s impossible to say precisely what’s going to happen. That said, there are signs that the flu’s hiatus is ending. And not only does it look like the flu could be back for the first time in three years, there are indications it could be a bad flu season.
INSKEEP: What indications do you mean?
STEIN: The big one is that after disappearing in the Southern Hemisphere for the last two years, the flu came roaring back in some countries south of the equator – in Australia.
INSKEEP: Oh. They’ve had their winter, so they’ve had their flu season. We’re getting an early sign here. OK. Go on.
STEIN: Exactly. Exactly. And in Australia, in their winter, the flu also hit unusually early. And what happens in the Southern Hemisphere’s winter often foreshadows what’s going to happen here.
Dr. William Schaffner is a flu specialist at Vanderbilt University.
WILLIAM SCHAFFNER: Clearly, the Southern Hemisphere had a serious influenza season. So if we have a serious influenza season and if the omicron variants continue to cause principally mild disease, this coming winter could be a much worse flu season than COVID.
STEIN: In fact, Steve, the CDC says the flu is already spreading in parts of the south, like Texas.
SCHAFFNER: This could very well be the year in which we see a twindemic (ph). That is, we have a surge in COVID and simultaneously an increase in influenza.
STEIN: And, you know, Steve, when it comes to the flu, it’s both the elderly and children doctors worry about most, especially this year.
INSKEEP: Why would doctors especially worry about kids?
STEIN: Well, you know, Steve, the big reason the flu basically vanished the last two years was everything everyone did to fend off COVID – you know, staying home, avoiding other people, you know, wearing masks, not traveling. That prevented flu viruses from spreading, too. And at the same time, the coronavirus may have kind of elbowed the flu out of the way. That helped spare us from an earlier twindemic, but it also means lots of kids have never been exposed to the flu.
I talked about this with Dr. Helen Chu at the University of Washington.
HELEN CHU: Because children haven’t seen flu for two years now, you have the 1-year-olds, the 2-year-olds and the 3-year-olds who have – all be seeing it for the first time, and none of them have any preexisting immunity to influenza. So I’m a little worried.
STEIN: The flu does appear to have hit kids especially hard in Australia.
CHU: Older children will get influenza. They will probably not get as sick as the younger children, but they’ll be the spreaders. They will then take it home to their parents. The parents will then take it to their workplace. They’ll take it to the grandparents who are in assisted living, nursing homes. And then those populations will also get quite sick with the flu.
INSKEEP: A pattern, of course, that we were warned about with the pandemic as well. But I want to note, I was in the other day to get a booster shot, and they said, get a flu vaccine, same time. And so I went ahead and got it – two shots. There are still good flu vaccines, right?
STEIN: Absolutely. Absolutely. So doctors are urging everyone to get a flu shot, which, so far, look like a pretty good match to the flu strains that are spreading the fastest right now.
Here’s Dr. Richard Webby at St. Jude’s Research – St. Jude Children’s Research Hospital.
RICHARD WEBBY: We should be worried. You know, I don’t necessarily think it’s run-for-the-hills worried, but we need to be worried enough to go out and get the vaccine. And my suggestion is get the vaccine probably early this year.
STEIN: Like you, like, get it now, Webby says. But experts are worried about that, too, because vaccination rates are down because of all the anti-vaccination sentiments stirred up by the pandemic.
INSKEEP: Well, what else can people do?
STEIN: The hope is that certain aspects of our new normal could help.
I talked about this with Alicia Fry at the CDC.
ALICIA FRY: The wild card here is we don’t know how many mitigation practices people will use. For example, people now stay home when they’re sick instead of going to work. If they keep their kids out of school, if schools are stricter about not letting kids come to school if they’re sick – all of these types of things could reduce the transmission.
STEIN: And could help prevent, or at least blunt, a twindemic.
INSKEEP: NPR’s Rob Stein, thanks.
STEIN: You bet, Steve. Transcript provided by NPR, Copyright NPR.
Alaska Native Medical Center nurse Rocky Carloni rolls up her sleeve before getting a COVID-19 booster shot. (Nat Herz/Alaska Public Media)
State health officials are encouraging Alaskans to get updated COVID boosters and flu shots ahead of flu season.
The new bivalent booster — which increases protection against both the omicron variant and the original coronavirus — has been available for nearly two weeks. In a public health presentation Wednesday, state epidemiologist Sarah Aho said approximately 8,000 doses have been given so far.
“That’s not a huge number. We’re hoping for lots more in the coming months,” she said. “And if you compare that to people who’ve received the primary series in Alaska for the COVID vaccine, that’s over 440,000 people.”
The state Department of Health is working with tribal organizations and local providers to get boosters and other medical supplies out to rural communities, including those in Western Alaska impacted by last weekend’s storm.
“Airports are in good shape, with just some minor problems in a few areas with lighting and such, so supply movement should be unhindered except normal Alaska weather,” said Gene Wiseman, section chief of rural and community health systems for the state’s Division of Public Health.
Health officials said COVID-related hospitalizations continue to go down in Alaska and across the country.
Epidemiologists are using hospital data to measure the severity of outbreaks rather than case numbers, since few at-home COVID test results get reported to the state.
Still, state physician Dr. Lisa Rabinowitz said getting boosted is worthwhile. In June 2022, unvaccinated adults were more than four times more likely to be hospitalized with COVID compared to those who’d had at least one booster.
“That tells us that vaccines continue to protect against severe illness, hospitalization and death,” Rabinowitz said.
Close
Update notification options
Subscribe to notifications
Subscribe
Get notifications about news related to the topics you care about. You can unsubscribe anytime.







9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))
