Book banning is not new — in the U.S. alone the practice goes back to Puritan times, when Thomas Morton’s book “New English Caanan” and others opposing this way of life were tossed from Massachusetts.
But the American Library Association said Monday that this year there have been more challenges to books than they have seen since they started tracking it in 2000.
The ALA’s Office for Intellectual Freedom counted 729 challenges to library, school, and university materials in 2021. It’s a significant jump: Last year the group noted 156 challenges — and in 2019, there were 377. Although the 2020 number was impacted by the pandemic, which forced schools and libraries to shut down, the ALA said they don’t usually get more than 500 book challenges in any given year.
And sometimes, those challenges contain more than one book title. The number of individual books challenged in 2021 totaled 1,597.
In a press release, ALA President Patricia Wong said: “We support individual parents’ choices concerning their child’s reading and believe that parents should not have those choices dictated by others. Young people need to have access to a variety of books from which they can learn about different perspectives.”
As part of the report, the ALA keeps a list of the top 10 banned books — pulled together from a variety of sources, including news stories and voluntary reports sent to the Office of Intellectual Freedom — that they say is not “exhaustive.” In fact, they say around 90% of book challenges remain unreported and receive no media attention.
Additionally, the ALA cannot track what they call “silent censorship,” when individuals take it upon themselves to make sure that books cannot be found in libraries — hiding them in drawers, tossing them out, or simply taking them off the shelves. This often leads to books being listed in library catalogues but never able to be found when looking for them.
This year, “Gender Queer” by Maia Kobabe tops the ALA’s 10 most challenged books list. The book, originally published in 2019 is set to be reissued in May. The ALA said that the memoir, done in comic form and recounting Kobabe’s path to gender-identity as nonbinary and queer, has been “banned, challenged, and restricted for LGBTQIA+ content and because it was considered to have sexually explicit images.” Many of the books banned and challenge in 2021 are related to LGBTQ+ topics and most were written by Black or LGBTQ+ authors.
For the last two years, “George” by Alex Gino topped the list; it’s not on the list this year.
The ALA points out that their recent surveys show that a majority of voters — on both sides of the aisle — oppose efforts to have books removed from their local public libraries.
“This poll demonstrates that, in fact, we are hearing from a loud local minority,” said Deborah Caldwell-Stone, director of ALA’s Office for Intellectual Freedom, who attributed the jump in numbers to organized campaigns and movements related to political groups. In fact, it’s a relatively new thing for the ALA to see elected officials challenging books, she added.
Earlier this year, NPR reported how these school issues have been front and center at local elections.
To counteract the campaigns challenging books, the ALA is launching a nationwide initiative meant to empower readers to fight censorship.
“Most libraries and schools have policies that say that people can certainly raise concerns about books. And we support that. That’s part of the First Amendment, the right to petition the government,” Caldwell-Stone said. “But there should be a process involved with that. There should be an effort to verify their claims about the book, to read the work as a whole, to determine whose information needs are being served by the books.”
10 Most Challenged Books of 2021
Here are the books the ALA tracked as most challenged in 2021:
1. “Gender Queer,” by Maia Kobabe — Banned, challenged, and restricted for LGBTQIA+ content and because it was considered to have sexually explicit images
2. “Lawn Boy,” by Jonathan Evison — Banned and challenged for LGBTQIA+ content and because it was considered to be sexually explicit
3. “All Boys Aren’t Blue,” by George M. Johnson — Banned and challenged for LGBTQIA+ content, profanity, and because it was considered to be sexually explicit
4. “Out of Darkness,” by Ashley Hope Perez — Banned, challenged, and restricted for depictions of abuse and because it was considered to be sexually explicit
5. “The Hate U Give,” by Angie Thomas — Banned and challenged for profanity, violence, and because it was thought to promote an anti-police message and indoctrination of a social agenda
6. “The Absolutely True Diary of a Part-Time Indian,” by Sherman Alexie — Banned and challenged for profanity, sexual references and use of a derogatory term
7. “Me and Earl and the Dying Girl,” by Jesse Andrews — Banned and challenged because it was considered sexually explicit and degrading to women
8. “The Bluest Eye,” by Toni Morrison — Banned and challenged because it depicts child sexual abuse and was considered sexually explicit
9. “This Book is Gay,” by Juno Dawson — Banned, challenged, relocated, and restricted for providing sexual education and LGBTQIA+ content
10. “Beyond Magenta,” by Susan Kuklin — Banned and challenged for LGBTQIA+ content and because it was considered to be sexually explicit Copyright 2022 NPR. To see more, visit https://www.npr.org.
The Food and Drug Administration will meet with outside advisers to talk about the next steps in formulating a COVID-19 vaccination plan. (Photo by Dinendra Haria/SOPA Images/LightRocket via Getty Images)
Most vaccinated people will probably require yet another COVID-19 vaccine booster shot in the fall, a top Food and Drug Administration official said Monday.
“That’s when we’ll probably have a fair amount of waning immunity in combination with likely further evolution of the virus, along with people going back inside,” where the coronavirus spreads more easily, Dr. Peter Marks, director of the FDA’s Center for Biologics Evaluation and Research, told NPR in an interview.
Marks says the U.S. must start planning now for whether everyone needs another shot and, if so, what kind of shot exactly.
“We could basically wait until another wave comes along and then try to make another vaccine and try to deal with it, but I think we know that doesn’t work, because we can’t manufacture and deploy vaccine fast enough,” Marks says.
The FDA is convening a special meeting of the agency’s independent outside advisers on Wednesday for a daylong meeting to begin to plan the next round of boosters.
The meeting comes about a week after the agency authorized a fourth shot — a second booster — for anyone age 50 or older to shore up immunity ahead of a possible new surge sooner than the fall. A more contagious omicron subvariant known as BA.2, which has fueled surges in other countries, is now dominant in the U.S., raising fears of another surge.
The tricky part of determining what do in the fall is determining what version of the coronavirus will be dominant by then, Marks says. It could be the omicron variant, but it could also be an entirely new variant. That raises doubts about just giving people a fifth shot of the current vaccine, he says.
“There is a certain diminishing return by giving the same vaccine over and over,” Marks says. “We have had enough evolution of this virus that it would make sense to want to try to cover some of the genetic diversity that has been introduced into the mix.”
One strategy would be to give people a new vaccine that specifically targets omicron or one of the other variants, such as beta, Marks says. Another option would be a new vaccine that combines at least two strains into one vaccine, which could provide even broader protection against any new variants that might emerge.
“By this fall, we may be on to a new variant. It could be sigma. It may be tau. There may be something new that may be circulating that we’ll have to deal with,” Marks says. “We’re going to have to make a good guess at what may be most effective.”
That’s how the flu vaccine is formulated each year, though the influenza virus is more predictable than SARS-CoV-2, the coronavirus that causes the disease COVID-19.
So far, an omicron version of the COVID-19 vaccine hasn’t produced very promising results in early testing. But scientists are waiting for more data about that shot and about other new versions of the vaccines that combine strains, such as omicron and the original strain, omicron and beta, or delta and omicron.
Another question is how often people will have to keep getting vaccinated moving forward.
“Will it be something like the yearly flu vaccine, or not?” Dr. Anthony Fauci, the White House science adviser, told NPR in an interview. “I have to emphasize: We don’t know the answer to that right now.”
Some experts worry that the FDA is just assuming another shot will be necessary, instead of focusing on the more important problem of vaccinating the unvaccinated and boosting the unboosted.
“The FDA agenda implies that, without open, transparent scientific discussion, … that repeated boosting is the way of the future. There has yet to be a discussion of the goals of boosting and the trade-offs,” Dr. Celine Gounder, an infectious disease specialist and senior fellow at Kaiser Health News, wrote in an email.
“People like to say we can walk and chew gum at the same time, but in a world of limited resources, there are choices and trade-offs to be weighed. What are we not doing at the expense of repeated boosting?” she says.
In a briefing document posted Monday, the FDA outlined the many questions that the advisory committee will discuss on Wednesday. One issue is whether the U.S. or the World Health Organization will take the lead in formulating the next version of the vaccine, as the latter does with the annual flu shot.
Unlike with the flu shot, regulators will need specific new data demonstrating that any new formulation of the vaccine is safe and effective, the FDA says.
Copyright 2022 NPR. To see more, visit https://www.npr.org.
Turning off the lights and closing the curtains isn’t exactly a catchy, new sleep hygiene hack, but this common sense advice is gaining even more scientific credibility.
Many Americans sleep in a room that’s punctuated with some form of artificial light — whether it’s coming from a TV, a jumble of electronics or an intrusive streetlight.
New research suggests that one night of sleep with just a moderate amount of light may have adverse effects on cardiovascular and metabolic health.
“I was surprised that even this fairly, I would say, small amount of light just getting through the eyes to the brain still had such notable effect,” says Dr. Phyllis Zee, senior author of the new study and director of the Center for Circadian and Sleep Medicine at Northwestern University.
The findings tie into a broader body of evidence that indicates being exposed to light at night may be harmful in a variety of ways and could predispose people to chronic diseases.
Physiological effects of light
The small, 20-person study conducted by Zee and her team at Northwestern was designed to measure the physiological effects of 100 lux of artificial light on healthy adults while they were sleeping.
“This is about enough light that you could maybe see your way around, but it’s not enough light to really read comfortably,” says Zee. For the study, all the participants spent their first night sleeping in a mostly dark room. The next night, half of them slept in a more illuminated room (the light was placed overhead).
Meanwhile, the researchers ran tests on the sleepers: they recorded their brainwaves, measured their heart rates and drew their blood every few hours, among other things. In the morning, they’d give both groups a big dose of sugar to see how well their systems responded to the spike.
The results, published in the Proceedings of the National Academy of Sciences this month, show several clear differences between the two groups.
Unlike those who spent both nights in the dark, the group exposed to the light had elevated heart rates throughout the night. They also had increased insulin resistance in the morning, meaning they had more trouble getting their blood sugar into a normal range.
Light can disrupt metabolism
Zee says there are multiple potential ways that being exposed to light at night could disturb our metabolism.
One possibility — supported by research — is that having the light on disrupts the quality of sleep, but surprisingly this study did not find that result while monitoring the people in the lighted room. In fact, the participants generally reported that they thought they slept fine.
The researchers also measured levels of melatonin, a hormone that helps with the timing of circadian rhythms and promotes sleep. Melatonin is typically suppressed during the day and rises at night.
Studies show artificial light at night can suppress melatonin levels, and scientists have found a link between the disruption of melatonin and several diseases, including cancer and diabetes. Though here, too, the study did not find evidence that melatonin levels were lower among the people sleeping with the light on.
“That probably means that the light level that was getting through the eyes was not really bright enough to suppress melatonin,” says Zee.
However, Zee and her team believe that this small amount of light was enough to activate the sympathetic arm of the autonomic nervous system — what’s responsible for the body’s fight or flight response. This is supposed to cool down during sleep as the body moves into a parasympathetic state, when the body’s heart rate and respiration decrease.
The changes in cardiovascular function suggest the small amount of light was enough to shift the nervous system to a more activated and alert state.
“It’s almost like the brain and the heart knew that the lights were on, although the individual was sleeping,” says Zee.
The study is an important example of how even relatively dim light exposure can be disruptive to our sleep-wake cycle, says Dr. Chris Colwell, whose lab at UCLA studies the mechanisms underlying circadian rhythms.
He says the findings makes sense because the autonomic nervous system has a robust daily rhythm.
“There’s a lot of coordinated actions that have to occur in order for us to get a good night’s sleep and the autonomic nervous system balance regulates that,” says Colwell.
This effect on the nervous system wasn’t “dramatic” — not as if the people were awake — but Colwell says it’s still concerning: “You don’t want that going on when you’re trying to get a good night’s sleep.”
Increased risk of chronic illness
The study’s findings that metabolic health suffered aren’t entirely surprising.
Colwell notes there’s already a solid pool of research, as well as large population studies, showing that disrupting circadian rhythms makes it harder to regulate blood glucose levels.
Some of these human studies have used a much brighter intensity of light — and not while people were actually sleeping. And while the findings of this study alone can’t predict what would happen in the long term, Colwell suspects the harmful effects would be cumulative: “This was only one night, so imagine if you’re living that way constantly?”
The body’s “master clock,” called the suprachiasmatic nucleus, is found in the brain, but organs and tissues throughout the body have their own cellular timekeeping devices. Cells in the pancreas that secrete insulin are one example. Disrupting the sleep-wake cycle can affect their ability to appropriately secrete insulin, which in turn controls blood sugar.
“That’s going to increase the risk of chronic diseases like insulin resistance, diabetes and other cardiometabolic problems,” says Dr. Charles Czeisler, chief of the Division of Sleep and Circadian Disorders at the Brigham and Women’s Hospital in Boston and a professor at Harvard Medical School.
For example, a large observational study of more than 40,000 women found that sleeping with a TV or light on was associated with a 17% increased risk of gaining 11 lbs over the course of five years.
Czeisler’s own research has looked at the metabolic consequences of disruptions in circadian rhythms for longer than just one night.
In a recently published study, he and his colleagues conclude that the negative effects on metabolism observed in their study participants over the course of three weeks were primarily because of disruptions to circadian rhythms — not necessarily because of sleep deficiency.
“When we did not increase their exposure to artificial light at night, we did not see adverse effects of chronic sleep deficiency on glucose metabolism,” he says.
This is not to say that sleep deficiency doesn’t also have major adverse effects on health — it does — but he says it simply underscores the far-reaching consequences of being exposed to light at nighttime.
“People think that as long as they fall asleep and are unconscious, it’s not having physiological effects, but that’s simply not true,” Czeisler says.
Copyright 2022 NPR. To see more, visit https://www.npr.org.
A federal program intended to help low-income student loan borrowers, and eventually offer them debt cancellation, has failed to live up to its promise, an NPR investigation has found.
More than 9 million borrowers are currently enrolled in income-driven repayment (IDR) plans, which are designed to help people who cannot afford to make large monthly payments. The plans also promise loan cancellation ater 20-25 years. But documents obtained by NPR offer striking evidence that these plans have been badly mismanaged by loan servicers and the U.S. Department of Education.
NPR obtained two-dozen pages of internal department documents, including emails and, most notably, a previously unreported, 2016 review of student loan servicers’ struggles to implement IDR. The documents shed new light on the 2021 revelation that, at the time, 4.4 million borrowers had been repaying for at least 20 years but only 32 had had loans canceled under IDR.
The documents also offer surprising new revelations. For example, some servicers weren’t clearly tracking IDR payments and did not know when borrowers qualified for cancellation.
In all, these records paint a breathtaking picture of IDR’s failure, and cast a shadow over the federal student loan program. While the Biden administration did not make these problems, it must now address them as it weighs restarting repayment after a two-year pandemic pause.
In response to NPR’s request for comment, an Education Department spokesperson said on Friday, “Borrowers place their trust in us to make sure these plans work the way they were intended to, and we intend to honor that trust. We are aware of historical issues with prior processes that had undermined accurate tracking of eligible payments. The current situation is unacceptable and we are committed to addressing those issues.”
Some servicers had no idea when borrowers qualified for forgiveness
The Education Department offers several IDR plans that make similar promises: a manageable monthly payment (as low as $0) as well as loan cancellation after 20-25 years of qualifying payments. It is the servicer’s job to count how many payments a borrower has made and proactively notify them when they qualify for loan cancellation (after 240-300 payments).
But the previously unreleased 2016 review of servicers, conducted by the department’s office of Federal Student Aid (FSA), found that three servicers – PHEAA, CornerStone and MOHELA – did “not have an IDR forgiveness payment counter” to track borrowers’ progress toward cancellation.
The review notes that borrowers with accounts at PHEAA, for example, would have had to request a manual count of past payments to gauge their eligibility for cancellation.
Ultimately, this means some servicers didn’t know if borrowers qualified for cancellation unless they were asked, by borrowers, to do a labor-intensive records review.
“It is not on borrowers to be keeping two decades’ worth of records of how their student loan payments were made and whether each payment counted towards cancellation,” says Abby Shafroth, an attorney at the National Consumer Law Center (NCLC), a nonprofit that has previously called for reform of IDR.
The review’s executive summary makes clear the department had long harbored worries about its servicers breaking the promise of IDR, noting “concern regarding the accuracy of the payment counters with our servicers has been on FSA’s radar for some time.”
As such, Shafroth says, the Education Department also deserves blame. After all, Congress created the first income-based plans back in the early ’90s.
“It appears that [the Education Department] waited until the 20 years were up [and IDR borrowers were becoming eligible for debt cancellation] and then said, ‘Oh, we should probably make sure that the servicers are counting payments,’ ” Shafroth says.
“The department could have avoided this mess if [it] had done its job,” says Rep. Virginia Foxx, the top Republican on the House education committee. “Year after year after year, Republicans and servicers have pressed the department to provide clear and concise guidance for how to manage this complex web of repayment plans, but the department has refused to do that.”
The documents also reveal other irregularities in how servicers count IDR payments.
For example, if a monthly payment of $100.01 is owed but a borrower pays just $100 – one penny shy of the required amount – three servicers (Great Lakes, Nelnet and Edfinancial) said they would still count it as a qualifying payment. But four others indicated they would not.
Borrowers with the lowest incomes are being hurt most
These internal documents reveal that servicers’ mismanagement of IDR is especially harmful for borrowers with the lowest incomes.
Under IDR, a monthly payment of $0 for a borrower earning less than 150% of the federal poverty line should still count toward loan cancellation. But in the same 2016 review, officials warned, these $0 IDR payments “that qualify for forgiveness are not adequately tracked.”
The documents do not explain “adequately” or the reason for the apparent failure.
“That is one of the most concerning things that you’ve highlighted because the people with the $0 payments are the folks in financial distress,” says Persis Yu of the Student Borrower Protection Center. “If that payment is not tracked adequately, it means that they’re in debt that they don’t owe. And to build a system in which we utterly fail the lowest income borrowers so explicitly is just inexcusable.”
Nearly half of all IDR borrowers are making $0 monthly payments, according to a 2019 analysis by the Center for American Progress (CAP). Not adequately tracking those payments could delay or derail millions of the lowest-income borrowers on their way to loan cancellation.
“We knew there was a problem,” says Rep. Bobby Scott, the top Democrat on the House education committee. “This is worse than we expected.”
Scott had requested a U.S. Government Accountability Office (GAO) investigation into IDR’s failings. The results of that GAO review are expected later this month.
“The idea that you haven’t counted certain payments is disturbing,” Scott says.
And that’s not the only failure hitting the system’s most vulnerable borrowers.
When borrowers default, their loans are transferred from a traditional student loan servicer to a new servicer that specializes in helping borrowers rehabilitate their loans.
But, these documents show, when borrowers return to good standing and to a traditional servicer, they also lose any record of qualifying IDR payments made prior to default.
This loss of past payment credit happens not because those payments no longer count (they do) — but because the technology is deeply flawed.
“That’s horrible,” says Beth Akers, who studies student loans at the conservative-leaning American Enterprise Institute (AEI). “There needs to be a safety net there. So let education work to allow people to, quote unquote, pull themselves up by their bootstraps. But when those bootstraps break or they’re not there, let’s make sure that there is something to catch them. And you know, in my mind, that’s IDR.”
Transferring borrowers between servicers is a game of telephone
You might expect it to be relatively simple to transfer a borrower’s financial information and payment history from one loan servicer to another.
But according to the documents obtained by NPR, moving borrower accounts is incredibly fraught. Borrowers’ information is transferred via what’s known as an EA27 file, and every time a file is transferred, data and context can be lost, and mistakes made.
In fact, earlier versions of the EA27 didn’t even include payment counts for certain IDR plans.
Transferring these borrower files is like a game of telephone: The more you do it, the more likely the message gets muddled.
As a result, when servicers inherit borrowers from other servicers, they often inherit records with holes. For example, the department’s 2016 review of one servicer’s records found glaring omissions in the accounts of transferred borrowers. Some records lacked basic information, like when a borrower changed repayment plans or how much the correct payment amount was.
(Illustration by Susan Haejin Lee for NPR)
With holes like that, a borrower could ask their servicer how far they are from debt cancellation, but would get a wildly wrong answer.
And all of these problems are compounded by the student loan system’s original sin.
Before the days of multiple loan servicers, there was simply one. From 1992 to 2009, ACS Education Services managed the entire federal student loan portfolio.
But when the federal government ended its contract with ACS and the company began transferring borrowers’ profiles to other servicers, it became clear that ACS had made a dizzying number of errors — more than 5 million according to a 2020 report.
ACS has alsofacedallegations of mismanaging IDR, misleading borrowers and of taking months, even years in some cases, to correct and update borrowers’ records.
Nearly every borrower who could be eligible for cancellation under IDR in the next few years was serviced by ACS at some point. That means their current records, including the count of their progress toward cancellation, could be built on the sand of erroneous data.
This matters now more than ever, after several servicers have ended their federal contracts and more than a quarter of all borrowers have been — or soon will be — transferred to new servicers.
What should happen now?
The good news is, some big, forward-looking changes have already been made or are in the works, including efforts to streamline cumbersome annual paperwork requirements.
While these reforms will help moving forward, they won’t do anything for the borrowers who have already been hurt by IDR’s past problems. That’s something the Education Department promised to address in its Friday statement to NPR, saying, “We will be making operational changes to get things right moving forward, and we will fix this for the borrowers who have been harmed by past failures with payment counting.”
“If you’ve made qualifying payments, you need to get credit for them,” Scott says. “And if the Department of Education has lost records, then the presumption or the burden of producing the records ought to be on the Department of Education.”
Not everyone believes the remedy should fall to the department.
“We’re not going to get these programs cleaned up without legislation,” says AEI’s Beth Akers, who supports the idea of IDR and blames lawmakers for creating such a difficult suite of programs to implement. “The servicers have a thankless job. So does the Department of Education, because they were handed a pile of garbage.”
Several advocacy groups, including The Education Trust and the Student Borrower Protection Center, have not only called for an IDR waiver but also substantial student loan cancellation for all borrowers, not just those hurt by IDR’s failings.
“We just need to recognize that there are these systemic failures — that, across the board, people are struggling to make these payments,” says Victoria Jackson, who studies higher education policy at The Education Trust. “And we can do that in a simple, straightforward way by having broad-based debt cancellation.”
Though that level of relief doesn’t sit well with Rep. Virginia Foxx.
“We don’t do that for people who borrow money to buy a car. We don’t do that for people who buy a home,” she says. “… So why should we treat loans for college differently than the way we treat loans for anything else?”
While there is disagreement about a remedy here, all agree: IDR has failed many borrowers.
Back in 2010, President Barack Obama celebrated the promise of income-driven repayment, declaring, “in the United States of America, no one should go broke because they chose to go to college.”
Twelve years later, the promise of IDR remains as powerful as it is unfulfilled.
Nicole Cohen edited this story for broadcast and for the Web.
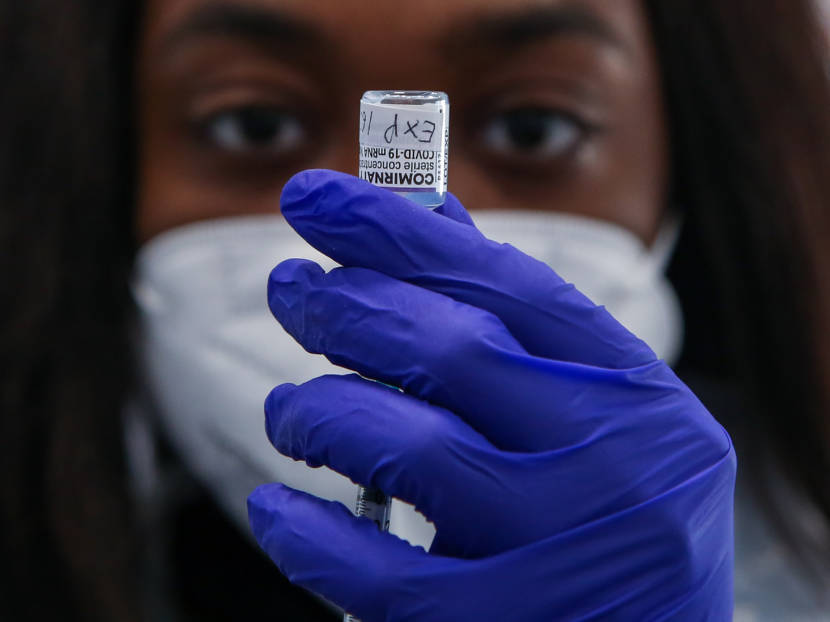
The FDA has authorized second booster shots for people over 50 and for some people who are immunocompromised. (Photo by Justin Sullivan/Getty Images)
The Biden administration has given the go-ahead for another COVID vaccine booster for people aged 50 and older and certain people who are immunocompromised. They can now get another Moderna or Pfizer-BioNTech booster at least four months after their last dose.
But just because you can get an additional booster, does that mean you need to?
Health officials argue that the protection provided by the COVID vaccine booster shots wanes over time. And they are concerned about people considered to be at highest risk of getting severe COVID.
But the Centers for Disease Control and Prevention didn’t make it clear how urgently people should be lining up for second boosters. The agency says these groups are “eligible” for the shots but it stopped short of saying they should get them. And some infectious disease experts say not everyone in this age group needs another shot now.
So, if you’re wondering whether to get a second booster, here are a few key factors to consider.
Risk of serious illness increases with age
Risk tracks with age, and older people have the highest risk.
A recent study among people 60 and older in Israel found that rates of COVID-19 infection and serious illness were lower in people who had a fourth dose of the Pfizer vaccine compared to three shots.
“We’re talking about extra protection from the most serious outcome of COVID,” says Dr. Eric Topol, founder and director of the Scripps Research Translational Institute.
Dr. Bob Wachter, chair of the Department of Medicine at the University of California San Francisco, says he personally plans to sign up for a second booster.
“I’m 64 and pretty healthy,” he says. “But the evidence is clear that six months out from my first booster shot, the effectiveness of that booster has waned considerably.”
He says another dose will boost his immunity and decrease the probability of infection. “The benefits are very real,” Wachter says.
But for people under 60 it’s less clear a second booster is necessary.
“I don’t think we have the data for younger people, 50 to even 60,” says Dr. Monica Gandhi, an infectious disease specialist at the University of California, San Francisco. The study out of Israel didn’t include this younger age group.
She points out that other countries are targeting additional boosters for older people. Germany has authorized a fourth shot for people over 70. The U.K. is targeting people over the age of 75 and Sweden is giving fourth shots to people over 80. Gandhi says the U.S. “is jumping the gun” by forging ahead with shots for everyone over 50 without the relevant data.
Still the trendline is clear, says Dr. Peter Chin-Hong, an infectious disease specialist at UCSF.
“The older you are, the bigger the benefit,” he says. Although the majority of deaths from COVID have been people older than 65, “there’s a clear association with age and mortality with COVID,” Chin-Hong says. “It’s really, really striking and it starts at age 50.”
His advice? “Walk to get the second booster if you’re eligible.” Then he says “walk a little faster the older you get.” His mom is in her 80s and he wants to protect her as much as possible. “I’m telling her to walk quickly,” he says.
Dr. Carlos del Rio, an infectious disease researcher at Emory University thinks it’s reasonable for people under 60 to wait. “The vaccines are holding up pretty well against severe disease and death,” he says.
It’s also worth noting that even for people over 60, the added protection of an additional booster shot, is small in absolute terms. People who got the first booster already have a very low risk of dying from COVID. Chin-Hong points out that in the Israeli study less than .1% of people with a third shot died, a risk so low he calls it “remarkable.”
Among people who got the fourth shot in this study just .03% died.
“Three shots is the magic number, we think, so far,” he says.
Underlying conditions put you at higher risk
Certain medical conditions also increase the risk of serious illness and death from COVID-19 and that’s the reason the FDA decided to authorize the additional boosters starting at age 50.
“We know that people in the age range from about 50 to 65 – about a third of them have significant comorbidities,” said Dr. Peter Marks, director of the FDA’s Center for Biologics Evaluation and Research, at a press conference Tuesday. People with heart disease, lung disease, obesity and diabetes are at higher risk for serious illness and death and people over 50 – particularly people of color – are more likely to have an additional risk factor.
“So by choosing age 50 and up, to consider those at high risk or higher risk,” Marks said. “We felt like we would capture the population that might most benefit from this fourth dose.”
When it comes to age, “there’s no bright cut off of risk,” agrees Wachter.
There are likely incremental increases in risk, year after year, as a person ages. A 50-year-old typically has lower risk than a 65-year-old, but health status matters, too.
“An unhealthy 55-year-old is probably at the same risk as a healthier 65-year-old,” Wachter says.
Bottom line, risk goes up with age and underlying conditions, and Wachter says many people over 50 may benefit from another dose.
“Anyone who has a serious medical condition, I would certainly suggest thinking about getting a booster,” says Dr. Preeti Malani, an infectious disease professor at University of Michigan Health. “For my own family, for my parents and my in-laws, this is something that I will recommend,” she says. “Because that extra layer of protection does help ensure that if they get COVID, it’s going to be milder.”
Immunocompromised people may need an extra boost
Health officials are particularly concerned about people who are immunocompromised because their immune responses to the vaccine tends to wane faster and they are at higher risk of getting severely ill or dying from COVID-19.
That’s why anyone 12 or older with certain immunocompromised conditions can now get an additional shot of the Pfizer-BioNTech COVID-19 vaccine, four months after their last dose. A second booster of the Moderna vaccine can be given to people 18 years of age and older.
This includes people who have undergone solid organ transplants, or who are living with conditions that have a similar level of immunocompromise.
Timing from last dose or infection is important
There is mounting evidence of waning vaccine protection against serious illness from COVID-19 in older and immunocompromised people, who are at least four to six months past their first booster.
Evidence of waning immunity comes from a recent CDC analysis of COVID-19 emergency room visits and hospitalizations visits during the omicron-predominant period. Two months after a third dose, people were 91% protected against hospitalization. But by four months, that protection dropped down to about 78%.
“It means that people who were boosted three, four, five, six months ago probably have limited protection against current infection,” Malani says.
This means a second booster can help shore up that protection, “but it’s not going to be long lasting.” So the timing of the additional shot can be tricky.
Right now the rate of viral infections has come down significantly since the peaks in January, but there are signs that infections are rising in some areas. The even more contagious omicron variant BA.2 is now the dominant variant in the U.S., and hospitalizations are also creeping up in some places.
Peter Chin-Hong says some people might want to wait to get a booster until a time when cases start to rise in their community and they need the added protection more urgently.
He also notes there may be more effective vaccines on the horizon. As vaccine makers test omicron-specific vaccines and continue research on vaccines that could fend off multiple variants, it may make more sense for people at lower risk to wait.
Still, if you’re high-risk, you may not want to wait too long. Polls show many vaccinated people held off on a first booster dose when they became available last year. But waiting until you see another outbreak in your community could be risky.
“It reminds me a little bit of trying to time the stock market. It turns out nobody’s actually good at it,” Wachter says. If there’s another outbreak on the horizon, it’s best to maximize your protection in advance of it.
There’s one more factor to consider when deciding on the timing of a fourth dose: Have you had a recent COVID-19 infection? If you’ve had three shots and you’ve had an omicron infection sometime between December and now, “I think it’s reasonable to wait.” Wachter says. He says a recent infection likely puts a person in a similar immunologic state as a second booster.
Rob Stein and Michaeleen Doucleff contributed to this report.
Copyright 2022 NPR. To see more, visit https://www.npr.org.
Through the pandemic, if you needed a coronavirus test, you could get one for free, even without insurance. Now, that is no longer the case in some places, as the federal funding covering the costs has run out. (Photo by Frederic J. Brown/AFP via Getty Images)
The first real-world consequences of dwindling federal COVID-19 funds have started to be felt in recent days.
Coronavirus tests for uninsured patients are no longer free in some places. That’s because the program that reimbursed clinics and hospitals for the testing, as well as for treating uninsured patients with COVID-19, stopped accepting claims last week “due to lack of sufficient funds.” Some clinics have already started to turn away people without insurance who come to get tested and can’t afford to pay for it.
Free vaccines for uninsured people are next — that funding will run out next week. After that, the vaccines themselves will still be covered by the government — for now — but the costs of administering them will no longer be billed to the federal program.
In another blow to the COVID-19 response, federal shipments of monoclonal antibody treatments to states — drugs designed to keep people infected with the coronavirus out of the hospital — were also slashed last week by 35%, according to Health and Human Services Secretary Xavier Becerra.
Biden administration officials such as Becerra warn that this is just the beginning. They’ve cited a long list of consequences — short and long term — as they plead with lawmakers to allocate $22.5 billion more for pandemic relief.
At the moment, that request for funding appears stalled in Congress. That has hospitals and public health experts worried that the U.S. will be poorly equipped to identify — let alone manage — whatever happens next with the pandemic.
As hospitals lose money, staff fear future surges
Losing this federal COVID-19 funding is “one additional threat” to safety net hospitals already strained by two difficult pandemic years, says Dr. David Zaas, who leads clinical care for the Medical University of South Carolina‘s network of 14 safety net hospitals in South Carolina.
He says that even without a pandemic, hospitals that primarily serve low-income patients run on tight margins. Add to that “the decreases in surgeries, as well as the increase in costs from the supply chain and labor, and the unpredictability of the different COVID waves,” and it’s clear why the pandemic has been so rough.
The Provider Relief Fund has been essential over the past two years, he says. His hospital network has gotten “$9.8 million of hospital reimbursement for predominantly inpatient care of uninsured COVID patients — that is now going away,” he explains.
He says the hospital network will continue to test and treat uninsured patients with COVID-19 and won’t bill patients for it, so the funding for that care will have to come “from the limited margin that hospitals generate to reinvest in our people and our programs and our facilities.”
The reduced monoclonal antibody shipments to states this week may also affect health systems and patients. Zaas’ health system has been providing those drugs to patients and even turned an old restaurant in a shopping mall into a COVID-19 infusion center. It’s unclear yet what the supply or cost of these drugs will be going forward, he says, though there’s also uncertainty about whether they’ll be effective against future variants.
The trade group representing Zaas’ health system — America’s Essential Hospitals — says these worries are being felt at hospitals that serve low-income and uninsured patients across the country.
“We are imploring Congress — and reaching out to the administration as well — to try to get at least some targeted financial relief to safety net institutions in the coming months,” says Beth Feldpush, senior vice president for policy and advocacy for America’s Essential Hospitals.
She’s worried, not just about whether hospitals will be reimbursed for caring for uninsured patients, but about whether there will be enough workers to provide that care. Health care workers are burned out by the pandemic, and many are leaving the field. Federal funding to help hospitals find, train and retain staff is drying up as well, she says, which is “really going to squeeze essential hospitals a lot over the coming months.”
Lost access to free care could fuel future outbreaks
As federal funds begin to dwindle, the strain on hospitals’ budgets and the reduced access to COVID-19 prevention and care for uninsured patients could have ripple effects.
There are 28 million uninsured people in the United States. If someone who’s uninsured is afraid to get tested for the coronavirus because of the risk of getting billed for it, the person might just not get tested when sick.
The person might also keep going to work in public-facing jobs, like serving food or driving an Uber. Zinzi Bailey, an epidemiologist at the University of Miami Miller School of Medicine, says all those hidden cases can drive more spread, with “bigger surges, different variants.”
“And we do not have this thing under control,” she says.
“We’re going back to common spaces. We’re going to be interacting. There’s no way to really divorce ourselves from people who may be uninsured,” Bailey says. Masks are also coming off, which makes it easier for the coronavirus to spread.
At the same time, the country might not notice if and when new surges begin — surveillance to detect and track new variants is also on the list of pandemic-fighting tools that are in danger of being cut.
“If we aren’t doing surveillance — either because we’re hoping for an end to the pandemic or because the money runs out and health departments and other institutions can’t afford to do it — then we are going to be caught unawares next time,” says Crystal Watson, a senior scholar at the Johns Hopkins Center for Health Security.
Already, at-home tests have made case counts unreliable measures of the true amount of virus in a community, and wastewater surveillance doesn’t cover the country evenly.
Boom-and-bust health funding continues
Watson is discouraged but profoundly unsurprised that lawmakers seem unwilling or unable to put more funding toward the pandemic.
“This looks like every other public health emergency that we’ve faced in the last 20 years,” she says. “Congress seems to get very fatigued of funding the emergency response, and so after people perceive that the acute emergency is over, they’re very quick not only to reduce funding but then to also really devalue the programs that are intended to prepare for the next emergency.”
But the cycle continues. Additional pandemic funding seems stalled in Congress.
One reason for the standoff is that Republican lawmakers have argued that they need a more detailed accounting of where previous COVID-19 funding has gone. At the White House’s first COVID-19 news conference in weeks, last Wednesday, health officials retorted that they’ve provided plenty of detail, and they even brought 385 pages of documents provided to members of Congress to prove it.
Gregg Gonsalves, an epidemiologist at Yale University who studies public responses to infectious disease, notes that the federal government’s messaging about how the pandemic is easing may be in part to blame for the impasse.
“I don’t understand how they can’t see the cognitive dissonance of the downplaying of the pandemic and then the need to get more money from Congress,” he says. “Either it’s a crisis and you need more money, or it’s not a crisis and you don’t need more money.”
He says even if cases are low, the country shouldn’t let up on surveillance, free tests and other efforts to keep the virus at bay. “You hope for the best and you plan for the worst,” he says. “You don’t just hope for the best, which is the national policy right now.”
In his South Carolina hospital network right now, Zaas says, there are only 43 COVID-19 patients across all their hospitals, but he’s still feeling nervous about what’s next.
“Even though COVID numbers are dropping around the country, none of us know what’s going to happen over the next six months,” he says. “I think all of us are worrying about an additional wave.”
Copyright 2022 NPR. To see more, visit https://www.npr.org.
Close
Update notification options
Subscribe to notifications
Subscribe
Get notifications about news related to the topics you care about. You can unsubscribe anytime.


9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))
9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))

9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))

9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))

9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))

9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))