Homer Port and Harbor officials say employees helped saved a vessel from sinking on Tuesday.
Early that morning, a harbor officer found the vessel Klahowya sinking and semi-submerged at its moorings and called for help, Deputy Harbormaster Matt Clarke said.
“He was able to install and implement emergency de-watering pumps before my arrival and was unsuccessful in saving the vessel,” Clarke said. “In further correspondence with him we realized that it was actually sunk and not achievable to successfully de-water based on the time that he had found it. So, we think it probably started taking on water and sinking somewhere in the neighborhood of 5 a.m. on Tuesday morning.”
The Klahowya is a 42-foot wooden motor sailor built in the 1940s, Clarke said.
He says the vessel sustained damage to its hull about a month ago and the owner told the port it was fixed.
The Klahowya was located adjacent to the Kachemak Voyager’s berth –- that’s the ferry that goes to Seldovia – and in the middle of two other vessels, which Clarke said helped save it.
“It was the middle vessel of a raft of three vessels so in a sense, when she began to sink and take on water, she was supported by the vessels mooring lines that it was tied off to on either side of her,” he said. “So, it did not sink to the bottom, it kind of started to reach a semi-submerged state.”
The adjacent vessels’ mooring lines, combined with the buoyancy of the Homer Harbor tug, which Harbor employees attached to the Klahowya’s stern, provided enough support to stabilize the vessel until the dive and salvage company arrived.
About 1 p.m., a diver positioned one air lift bag under the stern of the Klahowya and inflated it, which worked.
“We broke the gunnels in its stern and we were able to essentially plug all of the openings, the wholes the scuppers the through-hole fittings necessary to allow our three gas pumps, our two and three-inch gas pumps to commence rapid dewatering of the vessel,” Clarke said. “So once the gunnels were broke we had it beat and it wasn’t another hour or so until it was ultimately, entirely dewatered.”
The ferry’s berth was cleared by 1:30 p.m.
During the rescue the Seldovia ferry could not use its stall.
Homer Harbor staff cleared an alternate landing site about 400 feet away from her normal berth. The ferry was delayed about a half-hour.
The Klahowya is currently being monitored by Homer Harbor staff.
There are two auto bilge pumps on board now and the vessel is scheduled to be hauled out of the harbor to the boat yard on this Thursday afternoon.
Homer Port and Harbor officials are not releasing the vessel owner’s name at this time.
It’s a common scenario: Someone checks into a hospital for surgery or an illness and leaves with a prescription for an opioid painkiller, opening the door to long-term use and dependence. A recent study examined this pattern and found the prescriptions are used and renewed more often than you might imagine.
Researchers analyzed the pharmacy claims of a random sample of more than 623,000 Medicare beneficiaries who were hospitalized in 2011. They only included people who did not have a prescription claim for opioids for at least 60 days before being hospitalized.
The results, first published online in JAMA Internal Medicine in June, showed that 14.9 percent of the hospitalized beneficiaries filled a prescription for an opioid within a week after being discharged. Of those who filled the first prescription, 42.5 percent had another pharmacy claim for an opioid painkiller at least 90 days later.
“Presumably they were prescribed it and continued on it because of some sort of chronic pain,” said Dr. Anupam Jena, associate professor of health care policy at Harvard Medical School and the study’s lead author. Still, there are many ways to treat pain, Jena noted, and hospitals are supposed to look at other approaches.
In 2013, nearly 44,000 people died from drug overdoses, including more than 16,000 from opioid painkillers such as hydrocodone and morphine, according to the Centers for Disease Control and Prevention. Drug overdoses involving opioids nearly quadrupled between 1999 and 2013.
The JAMA Internal Medicine study found significant variations in the rate of new opioid use by Medicare beneficiaries across hospitals, from 10 percent on the low end to 20 percent on the high end.
In addition, hospitals that were ranked higher by patients for inpatient pain control had modestly higher rates of opioid use after discharge.
“For patients who are similar across a broad range of characteristics … there appears to be a large range in the propensity of hospitals to prescribe opioids,” Jena said. “The variation is alarming because it means some hospitals are doing it too much and some too little.” More research is needed to determine what the appropriate opioid prescribing standards should be, he said.
Please contact Kaiser Health News to send comments or ideas for future topics for the Insuring Your Health column.
KHN’s coverage of aging and long term care issues is supported in part by a grant from The SCAN Foundation.
President Obama speaks in Dallas in 2013 about the technical problems that affected the initial rollout of the Affordable Care Act. Now, citing the law’s success, he is urging Congress to expand the insurance offerings. (Photo by Brendan Smialowski/AFP/Getty Images)
President Barack Obama on Monday called on Congress to revisit the controversial idea of providing a government-run insurance plan as part of the offerings under the Affordable Care Act.
What’s been described as the “public option” was jettisoned from the health law in 2009 by a handful of conservative Democrats in the Senate. Every Democrat’s vote was needed to pass the bill in the face of unanimous Republican opposition.
But in a “special communication” article published Monday on the website of JAMA, the American Medical Association’s top journal, the president says a lack of competition among insurance plan offerings in some regions may warrant a new look.
“Now, based on experience with the ACA, I think Congress should revisit a public plan to compete alongside private insurers in areas of the country where competition is limited,” Obama writes.
The president calls on Congress to take more steps to rein in the cost of prescription drugs and make government assistance more generous for those who still cannot afford health coverage; he also urges the 19 states that have not yet expanded the Medicaid program under the health law to do so.
The public option has been a point of controversy from the start. It was included in the version of the health law passed by the House of Representatives, and had support from most Democrats in the Senate, before it was dropped. Many liberals hoped — and conservatives feared — that having the government provide insurance alongside private companies would be a step toward a fully government-run system.
On Saturday, as part of a deal with Sanders, Clinton announced she will also “pursue efforts to give Americans in every state in the country the choice of a public-option insurance plan,” which is broader than what Obama is endorsing.
But even if Clinton wins and the Democrats take back control of Congress in November, a public option remains a political long shot.
Obama’s article, titled “United States Health Care Reform: Progress to Date and Next Steps,” is apparently the first by a sitting president to be published by the prestigious medical journal.
Along with these recommendations for further action, Obama’s article includes a justification for the federal health law and statistics on how its implementation has improved insurance coverage for patients and improved health care quality.
Kristie Canegallo, the White House deputy chief of staff for implementation, says the article grew out of a comprehensive review of the law that the president requested from his staff late last year.
The review was to look at “what’s working, what’s not, and what we should do about it,” Canegallo says. Upon receiving the review, she adds, Obama “thought it was important to share some of this publicly.”
Among those parts of the law the administration says are working are the coverage provisions. “The number of uninsured individuals in the United States has declined from 49 million in 2010 to 29 million in 2015,” the president writes.
The article also says that the health law has played a substantial role in slowing the rate of health spending.
“While the Great Recession and other factors played a role in recent trends, the [president’s] Council of Economic Advisers has found evidence that the reforms introduced by the ACA helped both slow health care costs growth and drive improvements in the quality of care,” says the article.
Jason Furman, chairman of the council, says the continuing slow growth in health spending so many years out from the recession makes the argument by some other economists that the turndown in the U.S. economy was mostly responsible for the slowing of health spending “absurd at this point.”
While most of Obama’s journal article is a chart-driven, footnoted recitation of the impact of the health law, he does use his perch to suggest that the current state of politics in Washington threatens progress going forward.
“Any change is difficult, but it is especially difficult in the face of hyperpartisanship,” he writes. “Republicans reversed course and rejected their own ideas once they appeared in the text of a bill that I supported.”
Republicans are continuing their assault on the health law. Just last week, two House committees released a joint investigative report and held two hearings asserting that the administration is illegally providing funds to help lower-income individuals pay for their health coverage.
In states that made medical marijuana legal, prescriptions for a range of drugs covered by Medicare dropped. (Photo by Chris Hondros/Getty Images)
Prescription drug prices continue to climb, putting the pinch on consumers. Some older Americans appear to be seeking an alternative to mainstream medicines that has become easier to get legally in many parts of the country. Just ask Cheech and Chong.
Research published Wednesday found that states that legalized medical marijuana — which is sometimes recommended for symptoms like chronic pain, anxiety or depression — saw declines in the number of Medicare prescriptions for drugs used to treat those conditions and a dip in spending by Medicare Part D, which covers the cost on prescription medications.
Because the prescriptions for drugs like opioid painkillers and antidepressants — and associated Medicare spending on those drugs — fell in states where marijuana could feasibly be used as a replacement, the researchers said it appears likely legalization led to a drop in prescriptions. That point, they said, is strengthened because prescriptions didn’t drop for medicines such as blood-thinners, for which marijuana isn’t an alternative.
The study, which appears in Health Affairs, examined data from Medicare Part D from 2010 to 2013. It is the first study to examine whether legalization of marijuana changes doctors’ clinical practice and whether it could curb public health costs.
The findings add context to the debate as more lawmakers express interest in medical marijuana. This year, Ohio and Pennsylvania passed laws allowing the drug for therapeutic purposes, making it legal in 25 states, plus Washington, D.C. The approach could also come to a vote in Florida and Missouri this November. A federal agency is considering reclassifying medical marijuana under national drug policy to make it more readily available.
Medical marijuana saved Medicare about $165 million in 2013, the researchers concluded. They estimated that, if medical marijuana were available nationwide, Medicare Part D spending would have declined in the same year by about $470 million. That’s about half a percent of the program’s total expenditures.
That is an admittedly small proportion of the multibillion dollar program. But the figure is nothing to sneeze at, said W. David Bradford, a professor of public policy at the University of Georgia and one of the study’s authors.
“We wouldn’t say that saving money is the reason to adopt this. But it should be part of the discussion,” he added. “We think it’s pretty good indirect evidence that people are using this as medication.”
The researchers found that in states with medical marijuana laws on the books, the number of prescriptions dropped for drugs to treat anxiety, depression, nausea, pain, psychosis, seizures, sleep disorders and spasticity. Those are all conditions for which marijuana is sometimes recommended.
The study’s authors are separately investigating the effect medical marijuana could have on prescriptions covered by Medicaid, the federal-state health insurance program for low-income people. Though this research is still being finalized, they found a greater drop in prescription drug payments there, Bradford said.
If the trend bears out, it could have other public health ramifications. In states that legalized medical uses of marijuana, painkiller prescriptions dropped — on average, the study found, by about 1,800 daily doses filled each year per doctor. That tracks with other research on the subject.
Marijuana is unlike other drugs, such as opioids, in which overdoses are fatal, said Deepak D’Souza, a professor of psychiatry at Yale School of Medicine, who has researched marijuana. “That doesn’t happen with marijuana,” he added. “But there are whole other side effects and safety issues we need to be aware of.”
Study author Bradford agreed: “Just because it’s not as dangerous as some other dangerous things, it doesn’t mean you want to necessarily promote it. There’s a lot of unanswered questions.”
Because the federal government classifies marijuana as a Schedule I drug, doctors can’t technically prescribe it. In states that have legalized medical marijuana, they can only write patients a note sending them to a dispensary.
Insurance plans don’t cover it, so patients using marijuana pay out of pocket. Prices vary based on location, but a patient’s recommended regimen can be as much as $400 per month. The Drug Enforcement Agency is considering changing that classification — a decision is expected sometime this summer. If the DEA made marijuana a Schedule II drug, the move would put it in the company of drugs such as morphine and oxycodone, making it easier for doctors to prescribe and more likely that insurance would cover it.
To some, the idea that medical marijuana triggers costs savings is hollow. Instead, they say it is cost shifting. “Even if Medicare may be saving money, medical marijuana doesn’t come for free,” D’Souza said. “I have some trouble with the idea that this is a source of savings.”
Still, Bradford maintains that if medical marijuana became a regular part of patient care nationally, the cost curve would bend because marijuana is cheaper than other drugs.
Lester Grinspoon, an associate professor emeritus of psychiatry at Harvard Medical School, who has written two books on the subject, echoed that possibility. Unlike with many drugs, he argued, “There’s a limit to how high a price cannabis can be sold at as a medicine.” He isn’t associated with the study.
And, in the midst of the debate about its economics, medical marijuana still sometimes triggers questions within the practice of medicine.
“As physicians, we are used to prescribing a dose. We don’t have good information about what is a good dose for the treatment for, say pain,” D’Souza said. “Do you say, ‘Take two hits and call me in the morning?’ I have no idea.”
Kaiser Health News is a national health policy news service that is part of the nonpartisan Henry J. Kaiser Family Foundation.
Copyright 2016 Kaiser Health News. To see more, visit Kaiser Health News.
Garen Wintemute, director of the UC Davis Medical Center’s Violence Prevention Research Program, talks about gun control with journalists. (Cynthia H. Craft for California Healthline)
As the ancient Chinese proverb says, from crisis comes opportunity. That is certainly true for Garen Wintemute, a leading gun-violence researcher and emergency room doctor who finds “teaching moments” in the grief-filled days and weeks following mass shootings in America.
He is using a window of opportunity recently opened by the mass shooting in Orlando, Fla., to bring attention to the issue.
Wintemute, once named a “hero of medicine” by Time magazine, has led the Violence Prevention Research Program at the University of California, Davis Medical Center for 25 years. Twenty years ago, the federal Centers for Disease Control and Prevention abruptly stopped funding Wintemute’s program. He has since put up $1.3 million of his own money to keep it running.
Wintemute is one of the nation’s most prominent gun violence experts. He studies the problem from a public health perspective, using empirical research, and then proposes potential solutions based on his findings.
Wintemute’s projects are frequently controversial. His 1996 report on makers of “Saturday night specials” led California state legislators to ban the cheap handguns. Soon afterward, a firearms-manufacturer told him he had put a price on his head.
Wintemute also has proposed stripping the right to buy firearms from people convicted of violent misdemeanors — “a group sometimes referred to as not-so-law-abiding gun owners,” as he wrote in the 2013 book, Reducing Gun Violence in America.
California has adopted this proposal, but the federal government has not. To make his case to U.S. policymakers, Wintemute cites data showing individuals with just one misdemeanor offense — a non-violent one, at that — are five times more likely than people with no criminal background to commit firearm-related or other violent crimes.
He also points out the inherent dangers in plea-bargain arrangements, which can knock a violent felony charge down to a lesser misdemeanor sentence — thereby allowing a released parolee to pass federal background checks to buy guns.
Because of Wintemute’s work and advocacy, extremists send e-mail threats. Gun show dealers circulated a photo of Wintemute, advising firearms salesmen to “forcibly” throw him out if they spotted him. At the time, Wintemute was touring 78 gun shows nationwide — a self-described “guerilla scientist” masquerading as a firearms dealer to collect material for his 2008 book, Inside Gun Shows: What Goes on When Everybody Thinks Nobody’s Watching.
Recently, Wintemute delivered a bold challenge to his fellow physicians. In a research paper published in the Annals of Internal Medicine, he urged doctors to ask patients about their access to firearms, their knowledge of gun-safety, and injury prevention techniques. When Medscape.com posted a news story about it online, 700 comments flooded the site.
Wintemute sat down with California Healthline recently to discuss his life’s work and his reaction to the Orlando shooting.
Q: What was your first response upon learning that yet another mass shooting had occurred, this time in Orlando, killing or wounding 100 people?
My first thought is always about the pain and suffering that will forever be present for family members of those who lost their lives.
Q: Your next response?
I remind the public that deaths by mass shooting account for 1 percent of the people killed by firearms each year. Ninety people a day — day in and day out — die of gunshot wounds, suicides included.
Q: Were you surprised by the flood of opinions and comments that followed the publication last month of your research paper calling for physicians to ask their patients about guns?
I had no idea the proposal would be controversial. What I’d challenged physicians to do was to merely ask patients if they had access to firearms and if they knew how to handle them safely. After a detailed examination of federal and state government legislative language to discourage such lines of questioning, I found none actually outlawed such doctor-patient discussions. So, the paper detailed how physicians could go about structuring these conversations.
Q: Many experts consider gun violence to be a medical or criminal justice issue. Why should we view it through the lens of public health as you do?
Why wouldn’t it be a public health issue? David Satcher, head of the CDC 20 years ago, said, “If it’s not a public health issue, why are so many people dying?” There’s a war going on. Sandy Hook was a tipping point … People get angrier and angrier as this goes on. So we seek out data to identify who’s most likely to commit gun violence. I am an empiricist, a scientist driven by the evidence. This is the public health approach.
Q: What accounts for the increased frequency of mass shootings in the United States?
There are probably a half-dozen factors. There’s ISIS. There has always been hate in America. There’s alcohol and substance abuse. There’s despair, resentment over income equality. There’s more social distance among people. I’m convinced social distance is one of the reasons.
Q: Why is it important for policymakers to seriously consider the policy proposals you and your colleagues have drafted?
We are in dire need of policy overhaul in the United States. Experts, myself included, have closely studied and interpreted statistics showing alcohol abuse contributes to gun violence. In Orlando, witnesses said they saw the gunman drinking at the nightclub before leaving, only to return with his assault rifle and a revolver. Expanding policies that deny gun ownership to individuals with a record of alcohol-related offenses would likely lessen gun violence.
Q: After Orlando, the U.S. Senate again rejected legislation that would have tightened background checks and prohibited gun sales to people on a terrorism watch list. What do you make of that?
Some senators say the list has technical problems, is unreliable and possibly inaccurate. Fine. I say, make a better list. The larger problem is that we’re forced in all cases to make group judgments on eligibility to purchase firearms (felons, domestic violence misdemeanants, etc.). There are members of all these high-risk groups who won’t commit future crimes. We don’t know in advance who will, and who won’t. The only option is to have a policy that applies evenly to all members of the group.
Q: California has some of the tightest gun control laws in the nation. The state Senate, in response to the San Bernardino terrorist shootings last December, recently approved 11 more such measures. What impact will these have on keeping firearms out of the hands of the wrong people?
We’ll have to see them enacted, and then see what their effects will be. Some are not directed at restricting access. (Editor’s note: This interview took place before the full California legislature Thursday approved a package of gun control measures and sent them to Gov. Jerry Brown).
Q: What has your research told you about which populations are most at risk of injury or death by firearms?
Who knew that gun violence is an old white guy problem? Two-thirds of gun violence deaths are suicides. Firearm suicides are going up nationwide. Ninety percent of them occur among middle-aged to older white men, especially in rural areas with lower incomes and higher opioid use.
Q: What were the circumstances surrounding your loss of funding from the Centers for Disease Control and Prevention?
From 1989 to 1996, we received CDC funding. Then, the CDC cut grants specifically for firearms violence. Our research funding, my salary, disappeared. Congress had just outlawed using federal dollars for gun violence research. We turned to grants and private donors to close the gap. But there were still electric bills, gas bills and some staff salaries that research dollars would not cover. About 10 years ago, I decided the work we are doing here is really good and should be supported. I decided to keep the lights on myself and told staff, “You will be paid.” Over the years, I poured $1.3 million into the research program. I will continue.
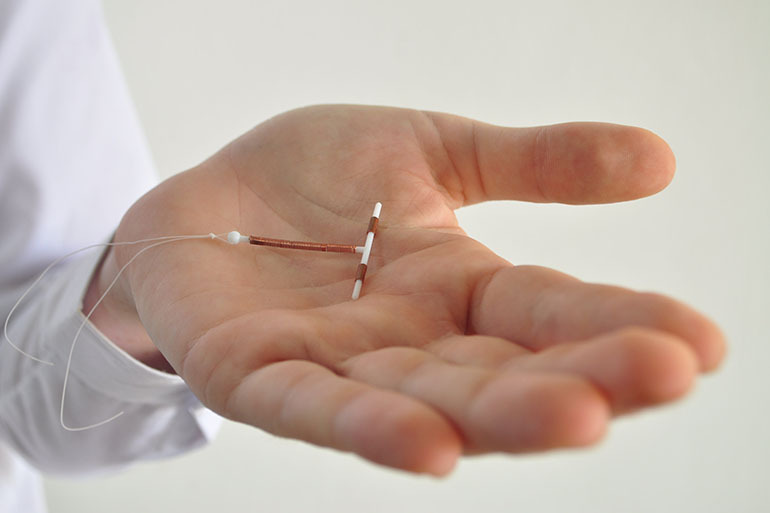
Medicaid spends billions on unintended pregnancies, and federal officials say better use of long-acting contraceptives, such as IUDs, offer advantages for women and are cost-effective. (iStock)
The federal government, which spends billions of dollars each year covering unintended pregnancies, is encouraging states to adopt policies that might boost the number of Medicaid enrollees who use long-acting, reversible contraceptives.
LARCs, as they are known, “possess a number of advantages,” Vikki Wachino, deputy administrator for the Centers for Medicare & Medicaid Services, wrote to state programs in a recent bulletin. “They are cost-effective, have high efficacy and continuation rates, require minimal maintenance, and are rated highest in patient satisfaction.”
And, Wachino stressed, “more can be done to increase this form of contraception.”
The federal push reflects the continuing concern over the nation’s rate of unintended pregnancies, which is one of the highest among developed countries. The costs are significant not only for the families involved but also for the federal and state governments. In 2010, the latest year for which data are available, the federal government spent $14.6 billion and states another $6.4 billion on unplanned pregnancies. (Southern states were especially affected. In Mississippi, public programs covered 82 percent of such pregnancies.)
LARCs are considered a key way to help reduce all of those numbers. They include intrauterine devices and under-the-skin hormonal implants that, once in place, provide nearly complete protection against pregnancy for three to 10 years. In contrast, birth control pills are about 90 percent effective and must be taken daily.
Under Medicaid, the state/federal health program for low-income people, states must cover family planning services for women and men without charge. Although they have considerable latitude in determining which services, they’ve generally included most methods of birth control, said Adam Sonfield, a senior public policy associate at the Guttmacher Institute, a research and advocacy organization that focuses on reproductive and sexual health.
Yet overall adoption of long-acting contraceptives has been slow in state Medicaid programs. In 2012, about 11 percent of low-income beneficiaries used a LARC, similar to the percentage of U.S. women overall.
Access in programs can be hampered by policies related to how LARCs are paid for and how services are provided, the CMS bulletin noted. It highlighted how some states are making changes to expand LARC use.
For example, it often is more efficient for a woman who has just delivered a baby to have an IUD inserted while she’s still at the hospital rather than wait until a postpartum visit several weeks later. But providers generally receive a bundled payment for labor and delivery services under Medicaid — and that doesn’t include IUD insertion. A dozen states — Alabama, Colorado, Georgia, Illinois, Iowa, Louisiana, Maryland, Massachusetts, Montana, New Mexico, New York and South Carolina, according to the CMS bulletin — have implemented policies that now reimburse providers separately for inserting an IUD or hormonal implant right after a woman gives birth.
Another hurdle is the high up-front cost of long-acting contraceptives. This can be addressed by increasing payment rates to doctors as an incentive for them buying and stocking the devices, the bulletin noted.
Some state programs require that Medicaid participants first try a different contraceptive method before moving to a LARC, a practice referred to as step therapy. Or they require a plan’s prior authorization, which can delay or even block women from getting that method. Both minimize use.
South Carolina, which in 2011 had the 12th highest teen pregnancy rate in the country, became the first Medicaid program to change its policy to reimburse providers for placement of LARCs immediately after delivery. The state now encourages the use of LARCs in outpatient settings by allowing the devices to be ordered by a physician but billed directly to Medicaid. In addition, it has eliminated prior authorization and step therapy as requirements.
The Center for American Progress, a liberal think tank, published a study last week calling for the increased use of LARCs for Medicaid enrollees both right after delivery as well as following abortion. It’s just one of a growing number of advocates, starting two years ago with the Association of State and Territorial Health Officials and continuing with the National Institute for Children’s Health Quality.
“The research is clear, LARC is the most effective and, over time, the least expensive reversible contraceptive method,” the nonprofits NICHQ and the the National Academy for State Health Policy stated in an issues brief last month. “Unplanned pregnancies are both medically difficult, with higher rates of preterm birth and low-birth weight babies, and incredibly costly. Wider adoption of LARC is a significant opportunity for states to reduce unnecessary expenditures in Medicaid programs.”
A recently published rule for managed care organizations that run many Medicaid programs also addressed LARCs. It said states must offer enrollees a choice of contraceptive methods and can’t require prior authorization or step therapy, said Mara Gandal-Powers, counsel for health and reproductive rights at the National Women’s Law Center.
“The language reinforces women’s access to the birth control method of their choice,” she said.
Read original article
Feds Urge State Medicaid Programs To Encourage Long-Acting Contraceptives
Close
Update notification options
Subscribe to notifications
Subscribe
Get notifications about news related to the topics you care about. You can unsubscribe anytime.



9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))

9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))