Bill Collins, police chief in Marion, Ohio, holds “blue drop” heroin laced with the painkiller fentanyl. Overdose deaths caused by fentanyl are surging. AP
When Ohio tallied what many already knew was an alarming surge in overdose deaths from an opioid known as fentanyl, the state asked the U.S. Centers for Disease Control and Prevention to investigate.
The rash of fatal overdoses in Ohio — a more than fivefold increase in 2014 — was not an isolated outbreak. Fentanyl is killing more people than heroin in many parts of the country. And the death toll will likely keep growing, said CDC investigators Matt Gladden and John Halpin at the fifth annual Rx Drug Abuse and Heroin Summit here.
Fentanyl, used in its legal pharmaceutical form to treat severe pain, represents the latest evolution of an epidemic of opioid addiction that began with prescription painkillers and moved to heroin, as users demanded cheaper drugs and greater highs.
At least 28,000 people died of opioid overdoses in 2014, the highest number of deaths in U.S. history. Of those, fentanyl was involved in 5,554 fatalities, a 79 percent increase over 2013, according to a December CDC report.
Unpublished data for the first half of 2015 indicate an even steeper spike in fentanyl deaths, Gladden said.
Cheap and Lethal
Fifty times stronger than heroin and a hundred times stronger than morphine, fentanyl is relatively cheap to produce illicitly and efficient to transport. It is often mixed with heroin, so that users are unaware they are inhaling or injecting the dangerous drug.
But after watching many of their friends drop dead over the last couple of years, most drug users say they are trying to avoid fentanyl, according to Traci Green, an associate professor of epidemiology at Brown University. Green was a panelist at the summit, presenting her findings from a study of fentanyl deaths in Rhode Island.
Users can sometimes detect fentanyl by color. It can be whiter than pure heroin powder, which typically has a brownish tint.
Still, some users seek out the powerful opioid for its superior high, Gladden said. “They find out someone just overdosed from it and they want to know where they can buy it.”
Because of its potency, the fast-acting opioid is more likely to cause an overdose than heroin or prescription painkillers. And fentanyl overdoses are more likely to be fatal: Because an overdose of fentanyl can shut down the lungs within two to three minutes of injection or inhalation, victims are less likely to be rescued than those who overdose on other opioids.
For suppliers of fentanyl, losing customers to fatal overdoses has not been a deterrent. Nor has drug users’ apparent fear of inadvertently using the deadly drug. When mixed with heroin, it creates a superior product that commands a higher price. Drug dealers keep producing it because it creates more addicts who are willing to pay for it, said the CDC’s Halpin.
The CDC’s analysis of Drug Enforcement Administration data revealed a twelvefold increase in law enforcement seizures of fentanyl since June 2013, primarily in Florida, Indiana, Kentucky, Maryland, Massachusetts, New Hampshire, New Jersey, Ohio, Pennsylvania and Virginia. This indicates a surging supply of the drug, which in some states already has propelled a significantly higher number of overdose deaths.
In 2014, drug overdose deaths jumped in many of the same states: New Hampshire (74 percent; all due to fentanyl, according to Gladden); Indiana (10 percent), Maryland and Massachusetts (19 percent); Ohio (18 percent); Pennsylvania (13 percent); and Virginia (15 percent), according to the CDC.
In Ohio, the agency found, the typical fentanyl-related overdose victim was a 38-year-old white male with a high school diploma and some college education. Many Ohio overdose victims had bipolar disorder, depression or other mental illnesses. And many had recently left a prison, jail, hospital or treatment facility. The deadliest month was April 2015, when 124 Ohioans died of fentanyl involved overdoses, the study found.
How to Respond
The CDC recommends that officials in Ohio issue warnings about the deadly street drug; intensify surveillance in the eight counties with the highest death rates; make the overdose-reversal drug naloxone more widely available; and ensure first responders are equipped with multiple doses of the antidote.
Because fentanyl is so potent, victims who overdose on the drug frequently require multiple doses of naloxone to be revived. They also need immediate follow-up treatment in a medical facility, making it imperative that bystanders call 911.
In general, the CDC calls for Ohio and other states to be more vigilant about testing for fentanyl in post-mortem toxicology reports to determine where fentanyl may be putting drug users at highest risk. Once fentanyl is detected, first responders in the area should be on high alert.
Long term, public health authorities and medical professionals should try to reduce the demand for fentanyl and other opioids through addiction prevention efforts, including safer practices in prescribing painkillers and improved systems for monitoring prescriptions.
Getting more people into treatment also will reduce that demand.
In Rhode Island, Brown University’s Green said, the state is sending recovery coaches to emergency rooms when people overdose to help them get into treatment. The next step, she said, will be to start overdose victims on addiction medication before they leave the hospital.
Tim Cullen, founder of Colorado Harvest Company, has had trouble keeping a bank account for his marijuana business. (Pew Charitable Trusts)
DENVER — Tim Cullen’s marijuana business brought in millions of dollars last year, but he’s had a hard time finding a bank to take the money. He’s cycled through 14 checking accounts in six years. Recently, he said, a bank shut down all his personal accounts, including college savings for his 3-year-old daughter.
Federal law prohibits banks and credit unions from taking marijuana money. So here in Colorado, everyone involved with the state’s legal cannabis industry has a banking problem. Businesses can’t get loans, customers have to pay in cash, and state tax collectors are processing bags of bills.
Some community financial institutions have become more open to serving the cannabis industry since the U.S. Treasury and Justice departments said they won’t go after institutions that keep a close eye on their clients and report suspected wrongdoing, such as funding gang activity.
But the big banks refuse to touch the industry, and banking challenges are only going to grow as legal marijuana expands. Nationwide, sales hit $5.4 billion in 2015, according to The ArcView Group, an analysis and investment firm that specializes in the legal cannabis industry.
Twenty-three states allow medical use of marijuana and four also allow recreational use. Voters in Arizona, California, Massachusetts and Nevada may legalize adult use this fall, and Vermont’s Senate recently approved a bill that would do so.
States are looking to Colorado — which legalized medical marijuana in 2000, and adult use in 2012 — for answers to the banking problem, but the state has few to offer. “We don’t truly think we’ll see a solution unless there’s a federal solution,” said Andrew Freedman, Colorado’s director of marijuana coordination, who’s also known as the state’s pot czar.
An Unbanked Industry
Cullen has been an unofficial spokesman for Colorado’s cannabis industry ever since he bumped into a CNN camera crew while picking up one of the state’s first retail marijuana licenses, he said. It helps that he’s a clean-cut former high school biology teacher who designed his stores with his mom in mind.
“We wanted to look like Restoration Hardware,” he said while walking through the main Denver location of Colorado Harvest Company, the marijuana growing and retail business he founded in 2009 and co-owns. That means wood paneling, edibles laid out in glass cases like chocolates, and a scent in the air that’s more reminiscent of a day spa than a college dorm.
But even Cullen’s squeaky-clean operation makes banks uneasy. The company’s current account, with a credit union, only covers basic services such as direct deposit for the company’s 70-odd employees and sending tax payments to the state, Cullen said.
An ATM sits in the corner of each of his three stores, because his business can’t process credit or debit card payments (credit card companies, like banks, may refuse to touch marijuana money). Every day an armored car swings by to pick up the day’s revenue — all cash — and takes it away to be deposited.
About 40 percent of Colorado cannabis businesses lack bank accounts altogether, according to the office of U.S. Rep. Ed Perlmutter, a Democrat who has pushed to improve banking for the cannabis industry. State officials would not comment on that number.
Freedman said a growing number of marijuana businesses seem to be obtaining bank accounts, judging by the declining share of tax revenue that businesses are paying in cash. But the services they’re able to access are limited and costly — “which means a lot of people prefer to keep as much as they can in cash,” he said.
All the cash floating around makes cannabis businesses targets for crime, Freedman says. Since Colorado fully legalized marijuana in January 2014, the Denver Police Department haslogged over 200 burglaries at marijuana businesses, as well as shoplifting and other crimes.
The loose cash also makes it harder for the state to track businesses’ finances to make sure they are obeying the law and paying their taxes. And in order to get a bank account, some businesses will funnel their cash through a shell company, Cullen said. “It starts to look a lot like money laundering.”
As Cullen’s experience shows, accounts can also be tenuous. Sometimes, a financial institution will change its mind about taking marijuana money. Or it might learn of a client’s ties to the marijuana industry. Mark Goldfogel, a consultant, said his bank closed accounts he’d held for 14 years after he revealed who his marijuana clients were.
Not Much States Can Do
Colorado’s attempts to solve the problem have shown other states how few options they have.
In May 2014, lawmakers authorized a new class of financial institution called a cannabis credit co-operative, which wouldn’t have to acquire and maintain deposit insurance. But no such institutions have been formed so far, partly because the Federal Reserve isn’t likely to approve them.
Later that year, lawmakers authorized a credit union for the cannabis industry. But the Fed denied the credit union access to a master account, which is necessary for transferring money, and the National Credit Union Administration refused to insure its deposits.
“Even transporting or transmitting funds known to have been derived from the distribution of marijuana is illegal,” the Federal Reserve Bank of Kansas City said during a court case the credit union brought and recently lost.
Without a master account, the credit union can’t fully function, said Mike Elliott, head of the Marijuana Industry Group, a trade association in Colorado. “It can be a vault. But we don’t need a vault,” he said.
Officials in other states that allow marijuana have run up against the same barriers. Tax officials in California have floated the idea of a state-run bank, for instance, as have officials inAlaska. But such an institution would still have to use federal wiring services, said George Runner of the California State Board of Equalization.
California already has trouble collecting taxes on medical marijuana, Runner said. “We’ve had folks come in with hundreds of thousands of dollars” in cash to make a payment. Other than increasing security at tax collection offices, there’s not much his office can do about it.
The cannabis industry’s banking problems would vanish if Congress were to take marijuana off the federal government’s list of most dangerous drugs. Last November, U.S. Sen. Bernie Sanders of Vermont, who is running for the Democratic presidential nomination, became the latest lawmaker to propose the change.
But that’s a remote possibility. Perlmutter has introduced a bill — twice — that would take a smaller step, and stop federal regulators from penalizing financial institutions for serving the cannabis industry. He hasn’t been able to get a hearing, let alone move the bill out of committee.
Perlmutter and his allies in Congress are now trying to cut off funding for federal enforcement actions against banks and credit unions that serve cannabis businesses.
Finding a Way
The Fed and other regulatory agencies have made it clear that states can’t create new financial institutions for the cannabis industry. But because the Obama administration has indicated that it will look the other way when existing institutions serve cannabis clients, businesses like Cullen’s do have some options.
Vermont’s Department of Financial Regulation has researched the services available to the state’s four medical marijuana dispensaries and found some good news. The state’s largest credit union serves one dispensary and says it would serve more. Although the credit union doesn’t offer marijuana businesses much more than depository accounts, federal regulators confirmed the accounts are insured.
Vermont state Sen. Joe Benning, a Republican who co-sponsored the Senate proposal to legalize marijuana for adult use, said the state’s financial institutions should be able to handle the cannabis industry’s expansion — at least initially. “You’re not going to have to be bringing in wheelbarrows full of cash to make deposits,” he said.
In other states, new services have emerged to eliminate cash transactions. In Washington and Oregon, an intermediary company called PayQwick electronically transfers money between marijuana growers, sellers, customers and their financial institutions. PayQwick also files all the paperwork the Treasury Department requires, taking a burden off banks.
Tax collection offices are doing what they can to manage cash collections. Offices in Oregon and Colorado have invested in extra security, such as safety glass and security cameras; businesses are also hiring security guards to help them make their deposits safely.
Auditing cash-only cannabis businesses is tough, but not impossible. In Colorado, the Department of Revenue relies on the state’s system for tracking legally grown and sold marijuana plants, Freedman said.
Still, the situation is far from ideal for businesses or for states. It’s temporary, too; nobody knows how the next president will enforce federal marijuana policies.
While Colorado waits for Congress to act, state officials will keep meeting with bank and credit union boards and explaining the nuances of federal law, Freedman said. That slow, institution-by-institution campaign may be states’ best hope for getting marijuana money off the streets.
“I think it’s going to get better. It certainly couldn’t be worse,” Cullen said of the cannabis industry’s banking problem. He takes the sunny view that as more states legalize the drug, it will become something federal lawmakers will no longer be able to ignore.
Makenzee Kennedy is groomed by nurse Megan Kelly in a special unit for weaning newborns off heroin and other opioids at North Baltimore’s Mount Washington Pediatric Hospital. The number of newborns suffering from opioid withdrawal symptoms has skyrocketed in the last five years. Getty Images
BOSTON — As soon as the home pregnancy test strip turned blue, Susan Bellone packed a few things and headed straight for Boston Medical Center’s emergency room. She’d been using heroin and knew she needed medical help to protect her baby.
“I felt so guilty. I still do,” said Bellone, a petite, energetic woman. At 32, and six years into her heroin addiction, having a baby was the last thing on her mind. “I was not in the right place to start a family,” she said. “But once it was happening, it was happening, so I couldn’t turn back.”
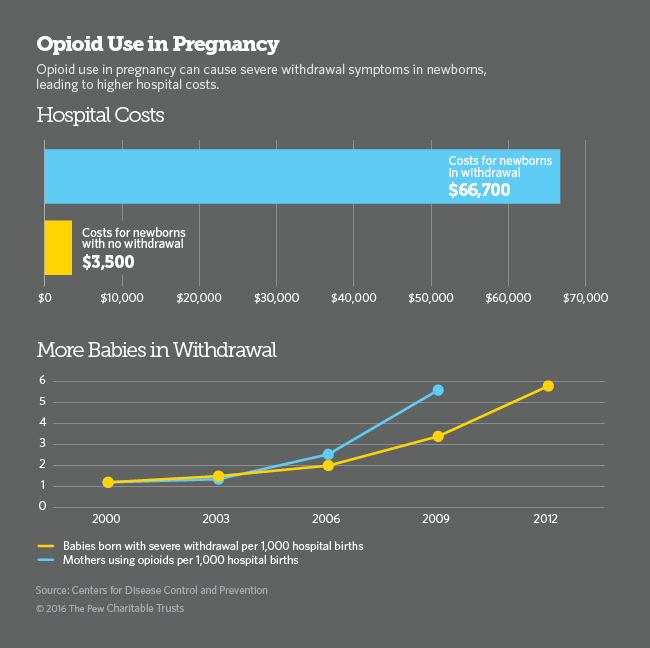
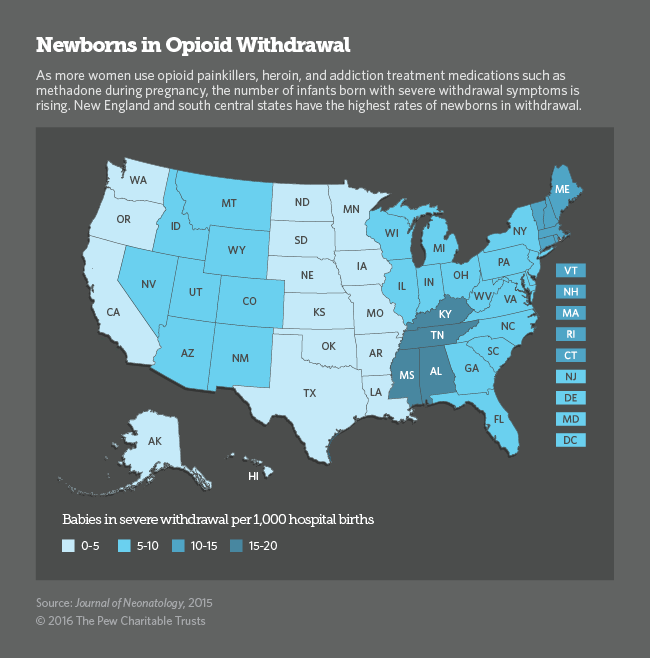
Nationwide, the number of pregnant women using heroin, prescription opioids or medications used to treat opioid addiction has increased more than five-fold and it’s expected to keep rising. With increased opioid and heroin use, the number of babies born with severe opioid withdrawal symptoms has also spiraled, leaving hospitals scrambling to find better ways to care for the burgeoning population of mothers and newborns.
Among the most important principles is that expectant mothers who are addicts should not try to quit cold turkey because doing so could cause a miscarriage. Trying to quit opioids without the help of medications also presents a high risk of relapse and fatal overdose.
Until the opioid epidemic took hold about eight years ago, most hospitals saw only one or two cases a year of what is known as neonatal abstinence syndrome. Now, a baby is born suffering from opioid withdrawal every 25 minutes in the U.S., according to the National Institute on Drug Abuse.
When a pregnant woman uses drugs or alcohol during pregnancy, some of the substances travel through the placenta to the baby. In many, but not all, cases, exposure to opioids during pregnancy can cause the fetus to develop physical drug dependence. When the umbilical cord is cut at birth, the newborn is abruptly disconnected from its supply of opioids and can suffer withdrawal symptoms.
When Bellone rushed to the emergency room six years ago, she didn’t know she’d gone to one of the best places in the country to receive addiction treatment during pregnancy.
At Boston Medical Center in the city’s South End, heroin addiction during pregnancy is not new. A specialized team of obstetricians, addiction medicine providers and counselors known as Project RESPECT has been treating pregnant drug users here for more than 30 years.
Now, dozens of hospitals and health clinics are gearing up to provide the same kind of specialized treatment for a rapidly rising number of pregnant drug users and their newborns
Although painful, newborn withdrawal symptoms, which include muscle cramps, tremors, diarrhea, vomiting, sleep problems and sometimes seizures, are not life threatening and have not been shown to cause health problems or developmental deficiencies later in life. The condition can be treated with small doses of morphine and subsides within a one to three weeks.
Methadone and Buprenorphine
As an epidemic of opioid and heroin addiction continues to ravage the nation, affecting at least 2.5 million people, hospitals and obstetrical practices nationwide have begun collaborating with addiction specialists to find the best way to treat women for their addiction while providing the safest care for their babies.
“Addiction specialists are terrified of treating anyone with a baby inside, and obstetricians are terrified of getting into addiction medicine,” said Dr. Ronald Iverson, of the Massachusetts Perinatal Quality Collaborative. But as demand for prenatal care for opioid-dependent women skyrockets, hospitals and private practices are increasingly offering combined addiction treatment and obstetrical services, so that pregnant women can see both specialists in one appointment.
Last year, a federal law was enacted — the Protecting Our Infants Act — authorizing the U.S. Centers for Disease Control and Prevention (CDC) to work with states to collect data on the prevalence of babies born with opioids in their bloodstream. It also calls on the U.S. Department of Health and Human Services to develop recommendations for the best way to prevent and treat drug use during pregnancy.
The standard of care for pregnant women using prescription painkillers or heroin is maintenance treatment with opioid addiction medications methadone or buprenorphine. Abstaining from drugs without medication is not recommended because of the high risk to the mother of relapse and overdose.
Although methadone and buprenorphine expose the fetus to low doses of opioids, the risk to the newborn of withdrawal symptoms is far outweighed by the risk of a fatal overdose when pregnant women receive no treatment or attempt to abstain from drugs without medication.
Abruptly quitting opioids in the first and third trimesters of pregnancy can cause harm to the fetus, including miscarriage and stillbirth, and is not recommended. Even in the second trimester, specialists agree that the risk of relapse outweighs any potential benefit to the fetus of lowering the dose of addiction maintenance medications or discontinuing their use.
Advocates for newborns, including the March of Dimes, agree with major medical organizations on the use of opioid treatment medication. But they argue more data and better research are needed to determine the best approach to treating opioid addiction during pregnancy.
“With pregnant moms, we’re weighing the high risk of death from overdose against the risk to the newborn of treating pregnant women with low dose opioid maintenance,” said Dr. Siobhan Dolan, medical adviser to the March of Dimes. With more research, she said, “we would be in a better position to consider abstinence and behavioral health counseling for some women.” And that could result in healthier babies.
According to the most recent data from the CDC, the number of opioid and heroin overdose deaths shot up by 14 percent between 2013 and 2014, killing more than 28,000 people, more than 10,000 of whom were women.
Fear and Misinformation
Most women who come into Boston Medical Center for drug treatment and prenatal care do so early in their pregnancy, said Dr. Kelley Saia, who heads Project RESPECT’s team that now treats about 250 patients at any given time, triple the number it did 10 years ago.
“They are so smart and so tuned into what they’re going through,” Saia said. “But they feel incredible guilt about taking medication during pregnancy and they worry about what their babies will go through.”
When Bellone arrived at Boston Medical she was ready to quit heroin. She’d done it before. “I wanted to stop everything. I didn’t even want to be on Subutex [a form of buprenorphine], but they said I might miscarry.”
On top of the normal worries about going through a pregnancy and becoming a parent, women with a drug habit worry about getting reported to child protective services. Massachusetts requires hospitals to report all babies born with opioids in their bloodstream to the state’s child welfare agency.
In many other states, doctors are required to report their patients to child welfare agencies before their babies are born, said Farah Diaz-Tello, an attorney with National Advocates for Pregnant Women, which advocates for the civil rights of drug-using women. In three states — Alabama, South Carolina and Tennessee — women can be prosecuted for child endangerment if they are reported using drugs during pregnancy. (The Tennessee law will not be in effect after July 1.)
Diaz-Tello and others say this threatens the health of women and their babies. Women need to feel safe so they don’t have to hide their drug use when seeking prenatal care or not seek care at all, she said.
Bellone said she wasn’t concerned about getting reported to child protective services because she knew she was doing the right thing. “If I wasn’t ready to quit I would have been worried,” she said. “But I knew five years before I got pregnant that I didn’t want to lead that life. I needed help and didn’t know where to go.
“It was almost like it took me getting pregnant to find help. It was hard to get into any place. There were no beds. But once you got pregnant it was instant, people were willing to help.”
Bellone’s pregnancy and her addiction treatment went smoothly. She delivered twin girls, Gemma and Mischa, on Aug. 3, 2010. They had to stay in the hospital for three weeks, but they’ve been healthy since they came home.
Perched on her chair sipping a huge to-go cup of iced tea in one of the hospital’s private consultation rooms, Bellone passed around photos of the twins jumping on their bed. Gemma, the oldest by seven minutes, just lost a tooth. “She pulled it out herself. She was very brave,” Bellone said.
Nearly six years after their birth, Bellone is still in recovery. She’s taking buprenorphine, making monthly visits to her addiction doctor and attending group meetings two times a week. She’s also working full time as a cook at a nursing home. “I’m tired a lot, like anyone with twins would be,” Bellone said. “People think I’m lying, but I never think about using.”
Is it in a child’s best interest to split time as evenly as possible between divorced parents? AP
It’s been about 40 years since the majority of moms stayed home, and married dads in the 21st century spend twice as much time caring for their children as they did back then.
Yet when parents divorce or separate, custody arrangements are more likely to reflect life as it was in 1975, with the mother as the primary caretaker and the father working to help support a child he seldom sees.
As fathers become more vocal about what they see as inequities in custody cases — and as more research shows how important it is for fathers to be present in their children’s lives — states are considering changing their custody laws.
Five states — Colorado, Florida, Maryland, Massachusetts and Missouri — are looking at proposals that would require judges to presume that it’s best for children to split their time as evenly as possible between their two parents. Utah enacted a similar law last year.
State laws have historically directed judges to determine custody based on what is in a child’s best interest, looking at factors such as which arrangement would disturb his or her life the least and be safest. The proposals would instead require judges to presume it’s best that both parents be awarded a substantial amount of parenting time — often at least a third of the time — and, if they don’t award substantial time to both parents, to explain why it wouldn’t be in the child’s best interest to do so.
Fathers’ rights groups, such as the National Parents Organization, are pushing the proposals, arguing that they will give fathers a better chance at a fair ruling and pointing to new research that shows how joint custody may be better than sole custody for children’s health.
But only a fraction of custody cases actually are up to a judge to decide — in Washington state, for example, nine in 10 cases that go to court are settled — and the cases that judges do hear are more likely to be ones in which parents can’t communicate or cooperate to make decisions. In those high-conflict situations, some researchers have warned that joint custody may be harmful to a child’s well-being.
Laws that encourage shared parenting may sound “seductive” to state lawmakers, but they often force families into bad situations, said Maritza Karmely, a professor at Suffolk University Law School in Boston. Bar associations, judges and lawyers have come out against some of the proposals.
“A presumption is a pretty radical step,” Karmely said. “That assumes that shared parenting works for most families, and I think that is an enormous assumption.”
But Ned Holstein, founder of the National Parents Organization, said none of the proposals forces judges to do anything. They would still be able to use discretion and decide what’s in the best interest of the child.
Changing Families
There haven’t been sweeping changes to state laws on custody arrangements since 1970, when the Uniform Marriage and Divorce Act set the “best interest” standard.
But the dynamics of American families have changed significantly since then. The share of children under 18 living with both parents fell, from 85.2 percent in 1970 to 69.2 percent in 2015. And more fathers are living away from their children, up from 11 percent in 1960 to 27 percent in 2010, a recent Pew study found; the shift is likely due to more children being born to unmarried parents. (Pew also funds Stateline.) At the same time, the amount of time married fathers spend caring for their children has more than doubled, from 2.5 hours a week in 1965 to 7.3 hours in 2010, according to Pew findings.
And that may be a good thing. Research shows that children who spend more time with their fathers are more likely to succeed academically and less likely to be delinquent or have substance abuse issues.
They will also grow up to be healthier mentally and physically, said William Fabricius, an associate professor of developmental psychology at Arizona State University who has been studying fathers and divorce since 2000.
In a yet to be published 10-year study funded by the National Institutes of Health, he found that children who felt they mattered to their fathers were less likely to later have mental health problems such as depression or anxiety.
“There are attributes and benefits that both parents bring to the child,” said Missouri state Rep. Kathryn Swan, a Republican who has sponsored shared parenting bills the last two years.
The Missouri Bar last year opposed provisions in Swan’s bill that put limits on judges’ discretion when deciding child support arrangements in cases where equal parenting time is granted; and that required judicial education on shared parenting. This year’s bill no longer includes those provisions, but the group has not yet taken a position on it.
Some fathers, such as Troy Matson of Jacksonville, Florida, push for shared custody, only to get worn down by the time, the cost and the acrimony of their court battles. Matson’s daughter was just a few weeks old when he and his wife started divorce proceedings. He asked to have her half the time. After contentious court hearings, the couple settled; he now sees his 4-year-old daughter 30 percent of the time.
Matson, who now chairs Florida’s chapter of the National Parents Organization, helped push a Florida bill that would require judges to presume that approximately equal time sharing is best. The bill, which passed the Legislature last week, would also require judges, when they rule differently, to show that equal time sharing is not the best solution. If Republican Gov. Rick Scott signs the bill, Florida would have one of the strongest shared parenting laws in the nation.
“I grew up without my father,” Matson said. “When I was a kid, I told myself if I’m ever blessed with children, I would do everything I could to be as involved in their lives as possible.”
Case-By-Case
Along with Utah, the National Parents Organization lists seven states as having laws most supportive of shared parenting — Alaska, Arizona, Idaho, Iowa, Louisiana, Minnesota and South Dakota.
While many family law and child psychology specialists agree that shared parenting is best in situations in which both parents are interested, involved and capable, they have concerns about other situations.
Domestic violence awareness groups have opposed some of the proposals, arguing that a victim shouldn’t have to prove that it’s not in a child’s best interest to live half the time with an abusive ex-partner. And specialists in the field have come to different conclusions about whether separating infants from their mother would be best for the infant’s well-being.
Most agree that each case is unique. “It is hard to find fault with examining each case and each child individually, when deciding what works best for their family and them,” said Peter Salem, executive director of the Association of Family and Conciliation Courts, a national trade association for family law professionals.
Fathers’ rights groups are often the ones pushing for the laws, but it’s not about the parents, said Robert Langlois, a former family court judge in Massachusetts who is now a lawyer there. “It’s about the kids, and what is in their best interest, not in their parent’s best interest,” he said.
When approaching a case, a judge looks at what the situation has been, if that should change, and why, Langlois said. Other factors judges look at include how old the children are, where they go to school, and where the parents live.
A bill proposed in Massachusetts would change the law to encourage shared parenting without requiring judges to presume equal time is best. Still, the change would require judges to provide reasoning when deciding a parent should not have significant time with a child.
“If you’re going to separate a child from one of his or her parents for most of their childhood, it’s only fair to say why,” said Holstein of the National Parents Organization, who lives in the state.
Outcomes
Proponents of shared parenting argue that current laws treat fathers unfairly. But gender bias in custody cases may be more perception than reality.
While mothers are custodial parents 82.5 percent of the time, it may just be because fathers aren’t asking for that job. A study in Massachusetts found that fathers who actively sought primary or joint custody obtained it more than 70 percent of the time.
In at least one state, specialists say recent changes to custody laws have made a difference. The Arizona Legislature passed a policy statement in 2011 in support of shared parenting and, in 2012, changed custody law to mirror the statement. This changed the culture of the court system, at least in Maricopa County, according to both Fabricius of the state university and Annette Burns, a lawyer there who specializes in family law.
The perceptions of parents have changed, too, Burns said. Now, both parents know they are likely to get a significant amount of time with their child.
A patient in the medical wing of the Kentucky State Reformatory in LaGrange. As the elderly population in state prisons keeps climbing, correctional systems are adding more services geared toward aging inmates, including hospice services and assisted living units. AP
CAPRON, Va. — Walter Melvin Atkinson is a bit vague about how long he has been in the assisted living portion of the Deerfield Correctional Center and how long he has left on his sentence. He claims to not even remember the crime — pedophilia — that landed him here.
At 92, “Speedy,” as he is called ironically by fellow prisoners and guards, is frail enough to require a wheelchair to get around, and his inmate caregivers rushed to his side to grab from his shaking hand a coffee mug that seemed destined to spill all over his cot. A huge, bright orange star has been sewn on to the white blanket that covers the cot — an idea the unit manager, Kathy Walker, dreamed up to help Atkinson spot his own bed among the six rows of beds in the spotless unit.
Atkinson is representative of an ever deepening trend in state corrections systems, and an ever growing problem, too. According to Human Rights Watch, from 2007 to 2010, the increase in the elderly population, 65 and up, being sentenced to state and federal prison outpaced the increase in the total population by 94 to 1.
Nearly every state is seeing that upward tick in elderly state prisoners. In Virginia, for example, 822 state prisoners were 50 and over (corrections officials usually consider old age for prisoners to begin at 50 or 55) in 1990, about 4.5 percent of all inmates. By 2014, that number had grown to 7,202, or 20 percent of all inmates.
For state prisons, the consequence of that aging is money, more and more of it every year. Health care for aging prisoners costs far more than it does for younger ones, just as it does outside prison walls. Corrections departments across the country report that health care for older prisoners costs between four and eight times what it does for younger prisoners.
In 2013, nearly half the $58 million that Virginia spent on off-site prisoner health care went to the care of older prisoners, according to Trey Fuller, acting health services director in the state Department of Corrections. “Over time,” Fuller said, “we’ll need more and more money for that population because they will need more drugs, more specialist visits, more nursing hours, more everything.”
Many states have taken steps to reduce their prison populations by releasing nonviolent inmates or by diverting some offenders to community programs before sending them to prison. But corrections officials say those reforms alone will do little to decrease the population of older prisoners who are serving mandatory sentences or have committed violent crimes.
Several states have adopted programs such as early release for geriatric patients or “compassionate release” for the dying. But advocates for prisoners say the programs are often so cumbersome and restrictive that few older prisoners are able to take advantage of them.
Accommodating the Elderly
The graying of the U.S. prison population reflects the rising median age of Americans since 1970. But that broader trend doesn’t fully explain the sharp increase in older prisoners. For that, corrections officials point to two factors. One is a steady increase in the rate of older adults entering prison. The second, and more potent, factor is changes enacted in the get-tough-on-criminals 1990s that resulted in longer prison sentences.
“It was the push for mandatory sentences and three strikes you’re out,” said Linda Redford, who studies health issues related to aging prisoners and is the director of aging and geriatrics programs at the University of Kansas Medical Center. “So we’re seeing people who came to prison in their 30s and 40s and 50s in their 50s and 60s and 70s today.”
Virginia’s problem was compounded in 1995 when the General Assembly eliminated parole for any offender entering its prisons from then on.
To accommodate the growing number of older prisoners, most states have been adding or retrofitting facilities.
“Prisons weren’t designed for patients who are getting older,” said Owen Murray, chief physician for Correctional Managed Care, University of Texas Medical Branch, which overseas health care for most of that state’s prisons. “They were designed for people 18 to 55” and who were able to walk, Murray said. One in five Texas prisoners is older than 50.
States have had to install ramps and shower handles and make other physical modifications. Many prisons have had to create assisted living centers with full-time nursing staffs, as Deerfield has. In addition, at least 75 U.S. prisons, including Deerfield, provide hospice services for dying prisoners, according to the Vera Institute of Justice, a nonprofit that advocates for criminal justice reform.
In prison, services for the elderly are often stretched thin. The 57-bed assisted living unit at Deerfield is always full; there’s a waiting list to get in. The nearby 18-bed infirmary provides hospice services, but its beds are also needed for nonterminal acute care patients, such as inmates who have just had surgery and need special care while they recover.
As a result, Deerfield has tightened restrictions on which elderly patients can go to assisted living or hospice care. For example, it used to be that prisoners would be considered eligible for assisted living if they could not perform any one basic task such as bathing, dressing or walking, said Susan Wright, nurse manager of assisted living at Deerfield. Now, they must be unable to do two or three or them.
Worse Health
People sent to prison are generally less healthy than the general population, having abused drugs and alcohol or neglected their health for many years. Prisoners have much higher ratesof cardiac disease, high blood pressure, hepatitis C, diabetes and other chronic diseases than the general population. That is why corrections officials consider that old age comes much sooner for prisoners.
“The norm in prisons is to use 55-and-older as the metric associated with older prisoners primarily because the consensus is that our population is 10 years ahead, clinically,” of people on the outside, Murray said.
Prison is a particularly treacherous place to get old. Getting to a top bunk is difficult for many aging prisoners, as is climbing stairs. Hearing loss, dementia and general frailty can make it difficult to comprehend or obey rules. And being infirm in an institution full of young predators can make older prisoners vulnerable. “If there’s an old lion or gazelle,” said Phillip Wheatley, one of the prisoner caregivers who tends to Atkinson, “the young ones are going to take advantage.”
When aging prisoners do reach the end of their sentences, corrections officials often have a hard time placing them, even if they look beyond their state. “Private nursing homes don’t want to take elderly offenders who were murderers or sex offenders,” said Virginia’s Fuller. He is currently keeping a wheelchair-bound former prisoner in a hotel, where a nurse visits daily, “because we couldn’t find a home for him,” he said.
Atkinson seems likely to present a similar problem. He was sentenced to 27 years in 1990 for pedophilia, paroled in 2005, and taken back into custody in 2008 for entering a school in violation of his parole. Thanks to credit he earned for good behavior, Atkinson could be released later this year, but his criminal record will likely make it difficult to find an outside assisted living facility or nursing home willing to take him.
Varying Approaches
Dealing with an aging prison population isn’t so complicated, said Texas’ Murray. “Either you figure out ways to get them out of the prison system and on to Medicare, or you choose to take a firm line that those patients have to do their time and you need to fund those facilities and care services that are necessary.”
So far most states have opted for the second approach, which means continuing to add services for an elderly population, including a special dementia unit for prisoners in New York state and housing units just for the elderly at Ohio’s Hocking Correctional Facility.
In 2012, Connecticut contracted with a private nursing home in Rocky Hill to care for elderly and infirm inmates granted parole. But even there, the state is locked in a battle with the federal government over whether the facility qualifies for Medicare or Medicaid reimbursement.
Several states have a mechanism they could use to shed some older prisoners. Louisiana, Ohio and Virginia have “geriatric conditional release” laws that make old age grounds for consideration for an early release. In Virginia, prisoners are automatically considered for release if they are 60 and have served 13 years or if they are 65 and have served five years.
Last year, 505 eligible prisoners were considered for geriatric release, according to Karen Brown, chairwoman of the state’s Parole Board. Only 3 percent were granted release, she said, adding that many of those who were denied had committed violent crimes.
Decisions about aging prisoners and the risk they would pose to the outside world should better reflect their medical conditions, said Brie Williams, an associate professor of geriatric medicine at the University of California, San Francisco, who studies aging in prison. “Health care professionals and criminal justice administrators should be coming together … to evaluate people for release,” she said. “We need to develop different approaches to their parole that are informed by their medical state.”
Virginia, like most other states, also permits the governor to grant clemency to prisoners certified by doctors to have less than 90 days left to live because of terminal illness. Last year,two Virginia prisoners received such clemencies.
Studies have found that older ex-offenders are less likely than younger ones to commit additional crimes after their release. But politicians and the public don’t seem willing to release former murderers, rapists and sex offenders, even though they are decades removed from their crimes and physically incapable of repeating them, said Liz Gaynes, president of the Osborne Association, a nonprofit that works on behalf of ex-offenders.
“It comes down to they did a bad thing and they should be punished,” she said. “Endlessly.”
States will be forced to pay more and more for that attitude, Gaynes said. “What to do about this is going to be the challenge for prisons in the next 20 years.”
An Oglala Lakota teenager sits in a juvenile detention center in Kyle, South Dakota. Native American girls are five times more likely than white girls to be incarcerated in juvenile facilities. The Washington Post via Getty Images
They’re poor, more likely to be sexually abused, end up in foster care, drop out of school, become homeless. They’re often the prey of traffickers.
American Indian and Native Alaskan girls are a small fraction of the population, but they are over-represented in the juvenile justice system, whether they are living on or off the reservation.
Native American girls have the highest rates of incarceration of any ethnic group. They are nearly five times more likely than white girls to be confined to a juvenile detention facility, according to the U.S. Office of Juvenile Justice and Delinquency Prevention.
There are programs on tribal lands that work with Native girls who have been caught up in the system, using federal funds. But American Indian girls often find themselves without state or local social service programs tailored to their cultural backgrounds and experiences, which are distinct from other girls living in or on the edge of poverty.
“As Indian people, our greatest hope is our children. And our kids are really at risk,” said Carla Fredericks, director of the American Indian Law Clinic at the University of Colorado Law School in Boulder. “The only way we can help these girls is if we do it cooperatively, with the states, federal government and within our own communities.”
A rare example of that kind of collaboration is the Minnesota Indian Women’s Resource Center in Minneapolis. In Minnesota, American Indian girls have 18 times the incarceration rates of white girls. They are often disconnected from family who themselves may be battling addiction and mental health problems. Native girls who are extremely poor and lack stable housing often get involved with gangs and drug and sex trafficking, said Patina Park, the center’s executive director.
The center’s programming seeks to combat those trends using a combination of state, federal and private funds to create culturally specific programs, including case management, support groups, housing and mental health services for American Indian women and girls and their families. The center also has youth-specific programming for girls ages 11 to 21, many of whom have been sexually assaulted, involved in sex trafficking or are at high risk.
The idea is to keep girls in school, off drugs and alcohol and focused on a future with a career, rather than turning to crime to make ends meet. The program, which is run with the help of the Fond du Lac Band of Lake Superior Chippewa, provides Native girls who’ve been cut off from their cultural heritage with a sense of community and purpose, Park said. Less than a quarter of American Indians live on tribal lands.
Since 1977, the White Buffalo Calf Woman Society on the Rosebud Reservation has been working with American Indian women and girls to address issues of sexual assault and domestic violence. Many Native juvenile girls are also victims of sexual abuse and family violence. But there are no such programs at the state and local level. Targeted programming coupled with more federal and state funding could make a huge difference in other cities and states with significant American Indian populations, Park said. “You could really change the disparity within the Native community fairly quickly and dramatically.”
Few Programs for Girls
Juvenile justice advocates who work with delinquent girls say they face challenges that boys don’t, and there aren’t enough programs that meet their needs. For example, girls are more than four times as likely as boys to have been physically or sexually abused, according to the National Women’s Law Center.
Delinquent girls are more likely than other girls to end up in the adult criminal justice system and are more likely to be dependent on social safety nets, according to Nona Jones of thePACE Center for Girls in Florida. They also are more likely to have children who end up in child protective services and the juvenile justice system. Girls who spend time in juvenile detention facilities are nearly five times more likely to die before age 29.
American Indian girls who collide with the juvenile justice system are particularly vulnerable, say legal advocates such as Terri Yellowhammer, an attorney with the Indian Child Welfare Law Center in Minneapolis who represents Native youth. Native girls are 40 percent more likely than white girls to be referred to a juvenile court for delinquency; 50 percent more likely to be detained; and 20 percent more likely to be adjudicated, according to the Office of Juvenile Justice. They are also more likely to face harsher sentences for the same offenses, said Joshua Rovner of The Sentencing Project.
American Indian girls in Wyoming have the highest rates of commitment to juvenile facilities (1,302 per 100,000), followed by Iowa (860), South Dakota (656), Oregon (568) and North Dakota (535).
In general, juvenile offender boys greatly outnumber girls, and that is true for Native boys, as well. But the disparities between American Indian boys and white boys aren’t quite as great.
Many Native girls are geographically segregated and isolated, particularly if they’re living in urban areas away from their communities, advocates say. They’re more likely than white girls to be arrested for crimes that are only crimes because they are underage, so-called status offenses, such as drinking alcohol or running away from home. They’re also more likely to be arrested for family disputes, Yellowhammer said.
And once they are arrested, they get tangled in a web of state, local and tribal jurisdictions, said Erik Stegman, executive director of the Native American Youth Center at the Aspen Institute in Washington, D.C. Law enforcement in Indian Country is uneven and exceedingly complicated, which hurts Native girls who run into trouble, he said.
According to the Tribal Court Clearinghouse, a database project of the Tribal Law and Policy Institute, tribal communities don’t have adequate funding to train law enforcement personnel and fund social service programs to combat juvenile delinquency.
Another complicating factor: Some tribes prosecute crimes and others do not, depending on tribal resources and capacity. As a result, Native girls often are prosecuted in the federal system, which doesn’t have a juvenile division. And if girls are arrested in the state system, the state usually doesn’t have to notify their tribes.
“We don’t have a system that’s nuanced enough to fit Native girls,” Yellowhammer said.
Stegman of the Native American Youth Center agreed: “When a young girl is traumatized, what she needs is a variety of interventions at the community level. Unfortunately, children end up bearing the brunt of a very haphazard criminal justice system.”
A Legacy of Trauma
American Indians today face a legacy of inherited trauma, legal experts say. Beginning in the second half of the 19th century, Indian children were shipped off to boarding schools far from their tribal communities and culture, in accordance with federal assimilation policies. Families were fractured.
The Indian Child Welfare Act of 1978 sought to right that situation, making it a priority to find homes for displaced American Indian children within their own tribe. In theory, the law is supposed to provide rights for families and tribes. But in practice, the law creates an extra layer of bureaucracy; with no one agency taking ownership of a child’s case, leaving children to languish in the system, said Sue Mangold, executive director of the Juvenile Law Center.
Children that grew up without parents become parents who don’t know how to raise children, juvenile advocates say.
In 2013, the American Indian and Alaska Native population was 5.2 million, about 2 percent of the U.S. population. The median age was 31, compared to 38 in the general population. And 29 percent of American Indians-Alaska Natives were poor, a higher rate than any other ethnic group.
American Indians ages 16 to 24 have the highest dropout rates in the country, more than twice the national rate, 15 to 7 percent. One in five Native girls become mothers before age 20.
American Indian women have the highest rates of rape in the country, more than twice that of other ethnic groups. The vast majority of the perpetrators are non-Indian men, according toAmnesty International.
All these factors create a climate where juvenile delinquency can flourish, child advocates say.
Violent crime rates among Native Americans are twice that of the country as a whole, and tribal communities experience high rates of domestic violence, child abuse and neglect, alcohol addiction and gang involvement, according to the Tribal Court Clearinghouse. Native children are over- represented in child protective services. And while the violent juvenile crime rate for U.S. teens has declined, it has increased for teens in tribal communities, according to the Clearinghouse.
A 2013 report by the Indian Law and Order Commission found that American Indian children suffer post-traumatic stress disorder at the same rates of veterans returning from combat duty in Afghanistan and Iraq.
“It’s like these kids are living in a war zone,” said Sarah Deer, co-director of the Indian Law Program at the Mitchell Hamline School of Law in St. Paul, Minnesota, and a 2014 winner of a MacArthur Fellowship, also known as a genius grant.
‘Blood Memory’
Working with Native girls who’ve ended up in the juvenile justice system in Minnesota has its challenges. Particularly girls who were lured into prostitution and peddling drugs by older men whom they believe to be their boyfriends and with whom they have developed intense, unhealthy emotional connections. Breaking those bonds is difficult, Park said.
Poverty shapes their lives in ways that makes it hard for them to see a way out, she said. To make ends meet, they often rely on “working long weekends,” heading out to the oil fields along the North Dakota border, “man camps” where men have cash and an appetite for paid sex. It’s tough trying to break them out of the cycle. “Sex is a tool for surviving,” she said.
But at the Indian Women’s Resource Center, they try. Young girls receive mental health services and education counseling. And elder women teach them about their cultural roots, learning about Indian medicine, ceremony, praying the traditional way and honoring their ancestors.
As Park sees it, these girls connect with the “blood memory” of their ancient heritage and heal from their past traumas.
“It gives them hope,” Park said. “It helps them see they can be more than their parents, who are struggling with drug addiction and homelessness. It’s hard to see yourself as more when you don’t see that around you.”