The mayor of Ithaca, N.Y., wants to create a place where people can use heroin or other drugs injected drugs under supervision, in an effort to combat soaring deaths from overdoses. But that’s a lot easier said than done.
The idea is that people addicted to heroin or other injection drugs would show up at the facility. They’re provided with clean needles, and trained medical staff stands vigilantly by with naloxone, an opioid overdose antidote, to prevent overdose deaths. Medical personnel don’t help users get high, but would give care and referrals to addiction treatment programs.
But since the drug use is illegal, both the city and staff risk breaking laws, too.
If Mayor Svante Myrick wants the injection site to see the light of day, there are major legal hurdles he’s going to have to surmount, says Leo Beletsky, a professor of law and health sciences at Northeastern University in Boston. The facility needs some kind of authorization or exemption from the state of New York, either by changing state law or as an executive action from the governor. Then Ithaca will need similar exemption at the federal level.
If Myrick can’t get any of those things, there’s another option he’s looking to pursue.
Mayor Svante Myrick of Ithaca, N.Y., says having a supervised facility for heroin users would reduce the toll on the community. Cliff Owen/AP
In 1992, the New York State Department of Health issued a state of emergency allowing public funding of needle exchange programs. “And they gave localities the power to make their own rules,” Myrick, who says his father was an addict, told Shots. “I think we’re in a similar state of emergency. We can’t wait any longer.” He hopes the state agrees.
Governor Andrew Cuomo’s office did not respond to a request for a comment on Ithaca’s plan. If no action comes from him and a medical state of emergency isn’t declared, there is one last, defiant option. Ithaca could go ahead with it anyway.
Similar things have been done in the past, Beletsky notes. “You have the entire [marijuana] industry in the U.S. that’s technically illegal under federal law, right? And yet it’s functioning.” The federal government is using its discretion not to go after people abiding by state law in states like Colorado, Beletsky notes, and that same concept could work on the state level. “Basically, if you play your cards right you can potentially do things that are illegal and yet are tolerated.”
In other words, Governor Cuomo doesn’t necessarily have to say yes. He just has to not say no. In a press conference Wednesday morning, Myrick said that he wouldn’t pursue that route. “We’ve no interest in putting time and money into something that will get shut down later.” But Myrick still has the option in his pocket, should he choose to take it out and create the first supervised injection facility in the United States.
Other countries have used safe injection sites for decades in an effort to reduce the death toll from heroin. The concept started in the 1980s in Europe. The first site to open in North America was in 2003 in Vancouver, Canada. After three years, the city showed large declines in people using injection drugs in public. Between 2004 and 2005, the medical staff made over 2,000 referrals for addiction treatment and other care a year. Researchers believe the Vancouver facility lowered overdose deaths by around 35 percent in its neighborhood and nearly 10 percent citywide.
But that doesn’t mean people in Ithaca aren’t worried. “Does Ithaca really need a government-run heroin shooting gallery?” writes William A. Jacobson, an Ithaca resident and Cornell University law professor, in his blog Legal Insurrection. “I have mixed feelings about such a location from a public policy perspective. The heroin scourge is real, I’m just not sure normalizing the use helps the problem.”
And Ithaca’s Chief of Police John Barber said in a press conference Wednesday morning that he disagrees with the creation of a supervised injection facility because heroin is still a controlled substance, although he does support other aspects of Mayor Myrick’s plan.
Other community members have said they want and will welcome the facility, according to Myrick. The idea to create the site came from Ithaca residents in the first place. “Over the course of the last two years, we compiled what people suggested,” he says. “And this plan is the response from the community.”
Figuring this out will take time. Myrick says he expects the facility to open in a couple of years.
Copyright 2016 NPR. To see more, visit http://www.npr.org/.
Read original article – February 24, 2016 2:58 PM ET
Health Commissioner Valerie Davidson testifies on a Medicaid reform bill in committee, April 15, 2015. Also pictured: Deputy Commissioner Jon Sherwood. (Photo by Skip Gray/360 North)
Medicaid is one of the biggest drivers of Alaska’s state spending.
At the same time, Alaska has the nation’s highest suicide rate and a growing problem with opioid addiction.
State leaders believe they can lower the long-term growth in Medicaid costs and make Alaskans healthier mentally and physically. They plan to do that by better coordinating behavioral health care — the treatment of mental health and addiction.
At a recent Senate Medicaid Reform Subcommittee hearing, Health Commissioner Valerie Davidson said it will be a challenge.
“This is hard stuff. If it was easy, Alaska would have done it long ago,” Davidson said. “And the great news is we have folks who have come together who are really interested in really changing the way that we deliver behavioral health services in our state, so that Alaskans can get the care that they need.”
In practice, it means more Alaskans will be screened for behavioral health issues in primary care settings, and a wider range of licensed counselors and therapists would be able to treat Medicaid recipients in a wider range of settings, like in a doctor’s office.
Davidson said current gaps in behavioral health care lead to other problems.
“We are seeing it in the number of children who experience child maltreatment,” she said. “And unfortunately, when we’re dealing with children, what we know is to the extent that that occurs, that can become a multigenerational issue. That if we don’t provide resources to family members who are in crisis, where we have places where they can actually go to receive help, we are never going to get ahead of this problem.”
A recent state-commissioned report recommended the state hire an organization that would increase the state’s capacity to provide behavioral health care, and manage a coordinated system.
While that organization would cost more than $5 million per year starting in 2018, the state projects that it would save a larger amount in future years.
Despite the state’s massive budget deficit, Anchorage Republican Sen. Cathy Giessel was on board.
“I appreciate the encouragement to invest in behavioral health and frankly I view it in the same way as investing in oil and gas credits for exploration. It pays off in the long run, though it costs a bit upfront,” Giessel said.
This coordinated approach is already practiced in some areas.
For example, Southcentral Foundation serves Alaska Natives with psychologists and social workers who treat patients in the same health centers as primary care providers.
The Alaska Mental Health Trust Authority board supports better integration of behavioral health care into the rest of the health care system.
Chief Executive Jeff Jessee said state leaders and providers will have to work together like a baseball team.
“The trustees believe this is the single biggest thing that the trust will encounter in our 20 years of history, this is an opportunity to truly transform our behavioral health and health care system,” Jessee said. “So, it’s the bottom of the ninth, we’re five runs down, we’re not bunting, and we’re not going to get one big swing either. We’re going to have to chunk away at this.”
While the groundwork for statewide behavioral health changes would happen over the next year under Gov. Bill Walker’s proposed budget, the bulk of the changes wouldn’t occur until 2018.
Two inmates likely going through painful opioid withdrawal in a jail in Portland, Maine. About 65 percent of the nation’s 2.3 million inmates are addicted to drugs or alcohol, but few get the medications that could help them beat their addictions. Getty Images
A week before 22-year-old Joe White was slated for release from the Barnstable County Correctional Facility, 26 law enforcement officials and social workers huddled around a table to discuss his prospects on the outside.
For substance abusers like White, they aren’t good.
In the first two weeks after a drug user is released from jail, the risk of a fatal overdose is much higher than at any other time in his addiction. After months or years in confinement, theoretically without access to illicit drugs, an addict’s tolerance for drugs is low but his craving to get high can be as strong as ever.
Most inmates start using drugs again immediately upon release. If they don’t die of an overdose, they often end up getting arrested again for drug-related crimes. Without help, very few are able to put their lives back together while battling obsessive drug cravings.
Barnstable, on Cape Cod about 70 miles from Boston, has broken that cycle with the help of a relatively new addiction medication, Vivitrol, which blocks the euphoric effects of opioids and reduces cravings. Such medications have been shown to be far more effective at helping people quit drugs than counseling and group therapy programs that do not include medication.
But even as the nation grapples with an epidemic of opioid overdoses, the use of medication to treat opioid addiction has faced stiff resistance: Only about a fifth of the people who would benefit from the medications are getting them.
The opposition is especially strong in prisons and jails. About two-thirds of the nation’s 2.3 million inmates are addicted to drugs or alcohol, compared to 9 percent of the general population, according to a study by the National Center on Addiction and Substance Abuse at Columbia University. Yet only 11 percent of addicted inmates receive any treatment.
White, whose story was relayed by Barnstable officials and who asked that his real name not be used, was a homeless substance abuser when he began a yearlong stint for stealing credit cards. He was set to receive a Vivitrol injection two days before he walked out — improving his chances of surviving long enough to get a second 30-day injection and some counseling.
Barnstable has been offering the medication to departing inmates for nearly four years. During that period, the recidivism rate among Vivitrol recipients has been 9 percent. That’s compared to a national re-arrest rate for drug offenders of 77 percent within five years of release, according to the Bureau of Justice Statistics. (Like many jails, Barnstable does not track its own recidivism rate.)
Beyond Barnstable
Since 2014, nine Massachusetts prisons and 10 jails have added Vivitrol to their drug treatment arsenals. About 50 state prisons in Colorado, Kentucky, Missouri, Pennsylvania, Tennessee, Utah and West Virginia now dispense the medication. And at least 30 jails in California, Illinois, Indiana, Kentucky, Maryland, Michigan, Missouri, New York, Ohio, Utah, Wisconsin and Wyoming also are offering it to departing inmates, according to the drug’s manufacturer, Alkermes.
The nation’s nearly 200,000 federal prisoners have not been offered any addiction medicines, though the Federal Bureau of Prisons is considering changing that policy this year.
Addiction experts argue medication-assisted drug treatment is not spreading fast enough in U.S. prisons and jails.
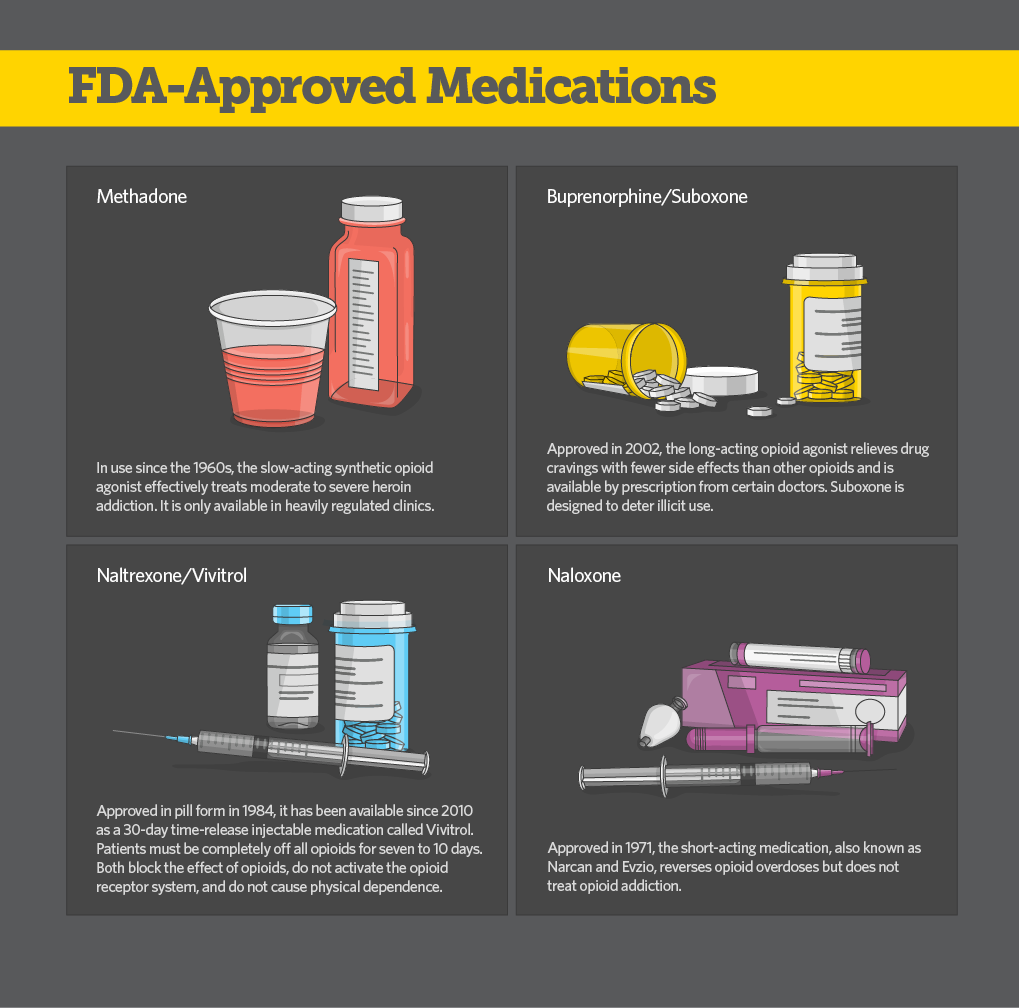
One of three medications approved for opioid treatment, Vivitrol is not a narcotic and therefore not a controlled substance. The other two medications, buprenorphine and methadone, are narcotics, which are anathema to most criminal justice systems.
The downside to Vivitrol is that patients must be off of all opioids for at least seven days before receiving an injection, a painful and sometimes costly proposition. Being behind bars obviates that problem, since most addicts do not have access to drugs while incarcerated.
Addiction specialist Dr. Kevin Fiscella said the failure to offer medication to more incarcerated addicts is “a missed opportunity” to treat inmates, many of whom are motivated to beat the disease that put them in prison, in a controlled environment. “There is no better place to intervene in an individual’s addiction than in corrections,” he said.
For one inmate at a Massachusetts prison, opting for Vivitrol was easy. In a video provided by corrections officials, he said he injured his shoulder playing lacrosse in high school and was prescribed Percocet, an opioid painkiller. He said he fell in love with the way it made him feel and quickly moved to heroin, a cheaper, more available alternative. Right after he graduated, he was arrested for breaking and entering and theft, and was sent to prison.
“I have friends that have sworn up and down about Vivitrol and how good it is and how it takes away the urge. They all have jobs now. They’ve been out of trouble forever. So when I got offered it, I said, ‘Don’t even finish the sentence, I’ll sign up right now,’ ” the inmate said.
Not a ‘Magic Cape’
Vivitrol is an injectable form of naltrexone, an oral medication that has been used to treat opioid addiction since 1984. It is similar to naloxone or Narcan, which reverse the effects of an opioid overdose.
Vivitrol and related medications, called antagonists, block the brain’s opioid receptors, making it nearly impossible to get high from opioids. Although scientists are not exactly sure how, antagonists reduce the addicted brain’s obsessive cravings for drugs.
Approved for opioid treatment by the U.S. Food and Drug Administration in 2010, Vivitrol was added to Barnstable’s longstanding re-entry drug treatment program in 2012.
Inmates who enter the program are told about the potential benefits of the medication and given the option of receiving their first injection a few days before being released.
“No matter how long they’ve been drug-free, inmates tell us they start actively dreaming about getting high in the last few weeks before they’re released,” Barnstable Sheriff James Cummings said.
Of the nearly 200 inmates who have chosen to receive the injection, about half have remained sober. Only one has died of an overdose.
“It’s not a magic cape,” said Andrew Klein, a corrections expert who is working with prisons and jails — including Barnstable — on medication-assisted treatment programs.
The biggest challenge, Klein said, is getting inmates to continue taking the medication once they leave the facility. “The physical symptoms of their addiction clear up pretty quickly and they feel like they’ve licked it, so they stop showing up for the monthly injections,” Klein said. “That’s when they tend to relapse.”
Experts agree that medications should be combined with behavioral counseling.
But the precise amount and type of counseling hasn’t been established. “At the very least, they need to be reminded to keep taking the medicine,” said Klein, a consultant withAdvocates for Human Potential, which specializes in behavioral health.
Although Vivitrol’s efficacy at dampening drug cravings has been shown, the drug is relatively new and no definitive study has proven its long-term effectiveness at preventing relapse.
Dosing and Counseling
At Barnstable, only 34 of the inmates who took Vivitrol completed an intensive six-month rehabilitation program before release. Despite agreement on the effectiveness of combining counseling and other types of therapy with the medicine, Barnstable does not require it.
“We’re seeing Vivitrol as a lifesaving medication,” said Jessica Burgess, the jail’s health services director. “We’re not going to deny it to anyone.”
Inmates interested in receiving it are given a physical exam. They also receive a short-acting oral form of the drug to check for potentially severe adverse reactions such as gastrointestinal disorders or dizziness. Inmates are also warned that once they are released, the long-acting medication will prevent them from getting high on opioids or alcohol.
On average, participants in the Barnstable program received five shots, including the injection they received before being released. Some stopped taking the injections after two or three months and relapsed. But according to Cummings, the sheriff, most were eager to get back on the medication.
Most ex-prisoners can’t afford to continue on the medication — which costs $1,000 per injection — without insurance coverage of some kind. In Massachusetts, prisons and jails enroll departing inmates in the state’s Medicaid program, which covers the cost.
Word of Mouth
Nearly half of the inmates in Barnstable’s 588-bed facility are addicted to opioids when they arrive. But in the nearly four years Vivitrol has been offered, fewer than 200 have opted to take it.
Their reasons for declining it vary. Most are in denial that they have an addiction. Many are unwilling to give up drugs and alcohol. Some don’t want to make the monthlong commitment that comes with receiving the injection.
But officials here say resistance is starting to diminish.
“The number of requests we’re receiving from inmates asking for Vivitrol has been steadily increasing since the start of the program,” Burgess said. “We attribute this to word of mouth and increased awareness.”
In the first year of the program, 37 inmates received the shot, followed by 51 the second year and 53 the third year. Since May 2015, 50 have signed up.
People outside of corrections who seek treatment for opioid and heroin addiction also have reservations about Vivitrol. Abstaining from opioids for seven days can be painful and dangerous. If patients relapse, they are at high risk for an overdose.
At Gosnold, a treatment center in nearby Falmouth, CEO Raymond Tamasi said the most common objection is fear of using drugs while on the medication and overdosing. That’s despite clear evidence that people who try to abstain from drugs without the help of medications are far more likely to die from an overdose, he said.
“Advances are coming in pharmacology,” Tamasi said. “Someday soon I expect we’ll view Vivitrol like the early days of penicillin.”
Thirty-three Alaskans died from heroin overdoses last year, a dramatic increase from just five years ago, when only four died. Another 54 Alaskans died of prescription pain-reliever overdoses in 2015.
Some of those deaths may have been prevented through the use of an opioid antidote, which can rapidly reverse overdoses.
Lawmakers are weighing a bill to make it easier for overdose victims to get the life-saving drug naloxone.
Some doctors feel comfortable prescribing naloxone. But others are wary of facing lawsuits related to drug overdoses.
That’s why state lawmakers are considering Senate Bill 23, which would provide civil immunity to doctors who prescribe naloxone, also known by the brand name Narcan.
Juneau resident Gary Miller’s daughter died last May from an overdose after taking heroin.
Juneau resident Gary Miller, whose daughter died from a heroin overdose, testifies in the Alaska House Health & Social Services Committee on Tuesday. He was supporting Senate Bill 23, which would provide immunity for prescribing, providing and administering opioid overdose drugs. (Photo by Skip Gray/360 North)
“I kept asking myself, what if I had done this, or what if I’d done that. Would she still be alive today?” Miller said during a hearing on the bill. “I finally had to stop doing that. I was driving myself insane doing that. But I can ask what would happen if this bill passes. There’ll be other parents who don’t have to go through what my wife and I went through. There’ll be other drug users who will get another chance at life.”
The bill would also give immunity to pharmacists who provide the medication, and people trained to administer it to overdose victims.
But bill sponsor Sen. Johnny Ellis, a Democrat from Anchorage, is considering widening the immunity to cover more people who could help overdose victims.
Naloxone can be injected easily into a person’s muscles. The federal Food and Drug Administration also approved a nasal spray form in November.
Naloxone is considered safe, which is one reason advocates for the bill want it to be widely available.
Christina Love is an advocate at Aiding Women in Abuse and Rape Emergencies, a shelter in Juneau. She said the legislature should act immediately.
Christina Love, a recovery coach from Juneau, testifies in support of Senate Bill 23. (Photo by Skip Gray/360 North)
“Expanded access to this life-saving drug would send a statement to the public: We are worth it, and every life matters,” Love said. “The only side effect of this drug is life. I can’t help but think if this bill would have been passed last year how many precious lives would still be with us.”
The bill also allows doctors to prescribe what’s known as a standing order to a pharmacy. This would allow the person who’s been prescribed the drug, a family member, or friend to pick up a prescription.
Dr. Jay Butler, the state’s chief medical officer, noted that in Rhode Island, pharmacies can dispense naloxone prescriptions to anyone who needs them.
Rep. Paul Seaton, a Homer Republican, encouraged Butler to do something similar in Alaska.
“The goal of everybody is to make sure that we have something safe and effective and available throughout the state, not just dependent on what … a local doctor and a local pharmacist would do,” Seaton said.
The Senate passed the bill 19-1 last April. The House Health & Social Services Committee recently held a hearing on the bill. The committee is scheduled to discuss the bill again on Thursday, and potentially vote on it.
Bill sponsor Ellis praised Seaton, the chairman of the committee, for focusing on a bill sponsored by a member of the other party.
“Rep. Seaton, to his credit, and his committee realize that this isn’t about normal procedure, or partisan politics,” Ellis said. “It’s a life-or-death, literally, a life-or-death situation.”
Ellis is hopeful the House will pass the bill and Gov. Bill Walker will sign it before the legislative session ends.
A woman at a Boston anti-drug rally wears a T-shirt showing family members killed by drug overdoses. As the country’s opioid epidemic worsens, few Americans are getting medication proven to be the best weapon against addiction. Getty Images
Dr. Marvin Seppala wrote a book on conquering drug addiction with counseling and group therapy.
The spiritual, abstinence-based strategy pioneered by Alcoholics Anonymous helped him overcome his own alcohol and cocaine addiction when he was 19. As medical director of Minnesota’s fabled Hazelden clinic, he watched it work for patients.
He believed in it — and then he changed his mind.
In 2007, Seppala began working at Beyond Addictions, a now defunct treatment center in Beaverton, Oregon. Instead of relying solely on counseling, the center gave its patients a relatively new medication, buprenorphine, to relieve their drug cravings.
Back in Minnesota, his patients had been bailing out of treatment to use illicit drugs again. In Oregon his patients on buprenorphine weren’t relapsing or overdosing — they reported feeling “normal” again.
Nearly a decade later, doctors and brain researchers agree that medications such as buprenorphine, methadone and naltrexone are the most effective anti-addiction weapons available. Nevertheless, more than two-thirds of U.S. clinics and treatment centers still do not offer the medicines. Many refuse to admit people who are taking them.
The result is that hundreds, perhaps thousands, of Americans are dying unnecessarily, victims of an epidemic that killed more than 28,000 people in 2014 — more than homicides and almost as many as auto accidents.
The research is unassailable: Staying in recovery and avoiding relapse for at least a year is more than twice as likely with medications as without them. Medications also lower the risk of a fatal overdose.
Addicts who quit drugs under an abstinence-based program are at a high risk of fatally overdosing if they relapse. Within days, the abstinent body’s tolerance for opioids plummets and even a small dose of the drugs can shut down the lungs.
And yet as the country’s opioid epidemic worsens — every day, more than 70 Americans die from overdoses, and the numbers are climbing — only about a fifth of the people who would benefit from the medications are getting them, according to a new study by the Johns Hopkins Bloomberg School of Public Health.
“When we discovered medications that worked for AIDS, deaths immediately plummeted. It became a chronic disease instead of a terminal disease,” said Dr. Andrew Kolodny, chief medical officer of the Phoenix House treatment centers, based in New York.
“This epidemic could be the same,” he said. “We have medications for addiction now. But unfortunately, we’re not making them available enough.”
People who could benefit from the medications are not getting them for numerous reasons. Among them:
Too few health care professionals have specialized training in addiction medicine. Although some primary care doctors have stepped in to fill the void, most are unwilling to treat patients with addictions and say they are often recalcitrant and disturbing to others in their waiting rooms.
Insurance coverage is limited. Few private insurers and state Medicaid programs cover all of the medications approved by the Food and Drug Administration. When they do, they typically limit the dosage or how long patients can take the medication or require them to first try group therapy, which is cheaper.
Many leaders of traditional drug treatment centers, such as national detox chains and residential rehab programs, are recovering addicts who conquered their own addictions without medication. They reject the notion that an addict can truly recover from a drug problem by becoming dependent on a different drug.
Greater use of medication could cut into the centers’ revenue, by reducing the number of people who opt for expensive residential stays. And smaller clinics that might want to add medication services would have to hire a physician to do so, which many of them could not afford.
Dr. Kelly Clark, an addiction specialist in Kentucky and president-elect of the American Society of Addiction Medicine, said some of the resistance is cultural, rooted in a widespread belief “that drug addiction is a moral failing, and that people should just get over it.”
“There is no other disease where approved medications are not provided to everyone who needs them,” Clark said. “We used to consider people with mental illness inferior, even possessed. Scientific advances have combatted stigma around a wide variety of brain diseases, but not addiction.”
Hazelden was one of the many treatment centers that resisted the use of medication — until Seppala returned from his stint in Oregon in 2009 and began pushing the board to shift course. Hazelden started offering the medications shortly thereafter.
“It’s hard to argue when you have patients dying of overdoses,” Seppala said. “We said this is truly a crisis, we can’t just base our service on philosophy, we have to look at the data and base our treatment on the best way to save lives.”
Freedom from Drugs
Opponents say addiction medications such as buprenorphine reduce drug cravings, but they don’t attack the underlying psychological problems that often go with addiction. Nor do they address shame, guilt and self-loathing — as counseling does.
Dr. Robert Mooney’s belief in abstinence has never wavered. As medical director at Vista Taos, a treatment center in New Mexico, he refers his patients elsewhere if they want to take medication. “What we do here is abstinence-based, because there are some people that nothing else will work on,” he said.
Mooney, a psychiatrist and board-certified addiction specialist, beat his own addiction to alcohol and cocaine with an abstinence-based approach, and he grew up in an abstinence-based treatment business. His parents, Dr. John and Dot Mooney, a surgeon and a nurse, overcame their own drug and alcohol addictions through abstinence and opened a treatment center, in Statesboro, Georgia, in 1971, to help others tread the same path.
“I tell patients, ‘We’re going to take you off all medications and give your brain a chance to land, and it’s going to be a long road.’ You need to prepare people for that.”
Mooney said he isn’t interested in arguing with those who believe in addiction medications, because in his view there has not been adequate research on the long-term effectiveness of either approach. “But let’s at least hang on to an abstinence-based philosophy, because we absolutely need it as part of the solution,” he said.
Seppala’s 2001 book, Clinician’s Guide to the Twelve Step Principles, embraces the approach first laid out in 1935 by Alcoholics Anonymous, “a fellowship of men and women who share their experience, strength and hope with each other that they may solve their common problem.”
He still says addicts who want abstinence-based treatment should get it. But, he said, medication should be offered. Like other addiction doctors, Seppala stresses that medication should be combined with counseling and group therapy whenever possible. Given the horrific toll of the drug epidemic, “We ought to put everyone on some sort of medication and give them all the psychosocial counseling we can,” he said.
The scope of the epidemic is staggering. Since 2008, more than 115,000 Americans have died from overdoses of prescription opioid painkillers and nearly 39,000 have died from heroin overdoses — reaching an overall death rate of 9 per 100,000 in 2014. That’s six times the drug overdose death rate of the 1970s, according to data from the U.S. Centers for Disease Control and Prevention.
New data from the CDC indicate the death toll from this epidemic has not yet peaked. Prescription opioid overdose deaths rose 16 percent from 2013 to 2014, to nearly 19,000. Heroin overdose deaths rose 28 percent and deaths from relatively new illicit opioids, such as fentanyl and tramadol, spiked 79 percent.
According to the U.S. Department of Health and Human Services (HHS), nationwide medication-assisted treatment capacity has increased somewhat in the past decade, but not enough to keep pace with the worsening opioid epidemic.
Many of the nation’s hardest-hit areas are rural and suburban. Rates of addiction are much higher in those areas and the shortage of providers is even worse.
“There are entire communities that are devastated by this epidemic,” Clark said. “If you have an opioid addiction, the odds are good that many, many in your world have the same disease. I’ve treated adolescents and their parents and grandparents.”
Nationwide, nearly 22 million people have some kind of substance use disorder, but only one in 10 goes to a treatment center, according to the most recent survey by the U.S. Substance Abuse and Mental Health Services Administration. In contrast, the treatment rate is as high as 80 percent for other chronic diseases such as diabetes, asthma, heart disease and high blood pressure.
Difficult Terrain
Addiction to opioids, including heroin and prescription pain pills, is difficult to treat. Not everyone recovers. Among those who do, most relapse at least once before entering a period of sustained recovery. For the millions of opioid addicts who are uninsured, homeless or recently incarcerated, getting on medication — and staying on — is a struggle.
But the affluent and the well-educated are also victims of this new epidemic. Their search for effective treatment can be frustrating and dangerous, their relapses frequent.
Kevin Flattery seemed to be in an ideal position to beat his addiction to OxyContin, a widely abused opioid painkiller.
After graduating from the University of Virginia, in 2010, Flattery moved to Hollywood to pursue his passion for filmmaking. Opioid painkillers were cheap and easy to acquire on the street there. Kevin tried them and liked them, in part because they relieved some of the stress he was experiencing as he pursued his high-pressure career.
Two years later, he realized he had an addiction that was taking over his life. Kevin decided to move back to his parents’ home in Mount Vernon, Virginia, an upper-middle-class suburb of Washington, D.C., to find help.
He had family support, financial means and no shortage of local treatment providers. But he got conflicting signals from the counselors he saw.
He checked himself into Inova Fairfax Hospital for detox, and the experts there suggested he start taking buprenorphine, one of the FDA-approved drugs.
The medication worked well for Kevin — at first. But he veered off course a couple of times, stopping the daily medication and buying OxyContin to get high. Each time, he got himself back on buprenorphine within a few days.
Experts say that’s a typical path for people who take such medicines. It often takes several tries before they stabilize and enter a period of sustained recovery.
But after a few months, Kevin wasn’t sure he wanted to stay on the medication for the long term. He attended local 12-step programs where he was criticized for taking it.
Kevin’s father, Don Flattery, said his son was confronted with judgment and pressure about it. “He was made to feel that he was not in recovery, not serious about his sobriety, and substituting one addiction for another — all utterly false but damaging to him nonetheless.”
Conflicted about how to proceed, Kevin stopped taking buprenorphine. Ten days later, he relapsed and suffered a fatal overdose, at age 26.
Three Medications
Buprenorphine and methadone are regulated as controlled substances by the U.S. Drug Enforcement Administration (DEA). Like the opioid painkillers that cause the addictions they are meant to relieve, both are commonly sold on the street.
But their euphoric properties are limited, making them poor options for getting high. The illicit use of methadone can cause a fatal overdose, particularly when combined with other drugs. But buprenorphine is relatively safe, even when used illicitly.
Methadone can cost less than $5 per day; buprenorphine costs about $10 per day. Although medical research has yet to establish standard lengths of time for using either, many have maintained recovery for decades on methadone. Buprenorphine has been used successfully for years by some, and only months by others.
A 2000 federal law requires doctors to seek a special waiver from the DEA to prescribe buprenorphine and limits their number of patients to 30 in the first year and to 100 in subsequent years. HHS may loosen the patient limit this year.
Methadone can only be dispensed by about 1,400 licensed clinics nationwide, both stand-alone and in prisons or hospitals. Most of them are in major cities, meaning the medication is unavailable to most in rural areas. Patients must show up every day to receive their dose under the supervision of a licensed professional.
Vivitrol, an injectable form of naltrexone, is not a narcotic and therefore not regulated. Instead of fulfilling the addicted brain’s perceived need for opioids, it blocks the effect of the drugs and thereby reduces cravings.
Any doctor can prescribe and administer Vivitrol. But it has a major drawback: To avoid severe and dangerous withdrawal symptoms, patients must completely detox from all opioids for at least seven days before receiving the first shot. For many, that means residential treatment, which can be costly. The drug itself is also expensive, at $1,000 per month.
Research on Vivitrol’s long-term effectiveness is still to come, but its use is spreading, particularly in jails and prisons. Patients are also increasingly opting for Vivitrol because the shots are effective for 30 days, tempering the temptation of stopping daily doses to get high.
Addiction doctors agree that all three medications should be available to patients, because one may be more effective than another, depending in part on the person’s age, length of time as an addict, home and work environment and underlying mental health issues. The American Medical Association, the American Academy of Addiction Psychiatry and the American Society of Addiction Medicine unequivocally support their use.
Patients should have a say in the kind of medication they want to receive, said Dr. David Gastfriend, scientific adviser to the Treatment Research Institute, in Philadelphia, which analyzes the effectiveness of addiction treatments. “They’ve heard about certain drugs from their friends or they’ve had past experiences and they often have ideas about what they want,” he said. “Treatment works much better with patient buy-in.”
Gastfriend and other addiction experts emphasize that medication should be accompanied by at least some counseling or group therapy. How long patients must stay on the medications remains unknown.
A Turning Point?
For advocates of medication-based treatment, recent policy changes are cause for optimism. The Affordable Care Act allows states to expand health insurance coverage to low-income adults and, for the first time, makes Medicaid and private insurance coverage of substance abuse treatment mandatory.
In the past, Medicaid only covered low-income pregnant women, children and disabled adults. Any drug or alcohol coverage was limited to those three populations. A severe drug or alcohol addiction, while debilitating and life-crushing, did not qualify on its own as a disability.
Under the ACA, 30 states plus D.C. have opted to expand Medicaid to low-income, able-bodied adults, giving millions of poor Americans coverage for addiction treatment. The health law also requires all state Medicaid programs and all insurance companies to cover the gamut of recommended treatments for addiction.
In addition, the federal Mental Health Parity and Addiction Equity Act, although not enforced everywhere, requires insurers to pay for proven addiction treatments at the same dollar level as medical and surgical treatment for purely physical diseases such as cancer.
“There has never been a better time to confront the addiction problem we have in this country,” said Michael Botticelli, director of the U.S. Office of National Drug Control Policy.
“We know so much more about addiction from years of scientific research. We know that substance use disorders are diseases of the brain, that they can be chronic and relapsing,” Botticelli said. “But we also know that like other diseases, they can be prevented, treated and people can recover.”
Suboxone pills. (Creative Commons photo by Supertheman)
Dr. Kelly Eagen witnesses the ravages of drug abuse every day. As a primary care physician at a public health clinic here in the Tenderloin, she sees many of the city’s most vulnerable residents.
Most are homeless. Many suffer from mental illness or are substance abusers. For those addicted to opioid painkillers or heroin, buprenorphine is a lifesaver, Eagen said. By eliminating physical withdrawal symptoms and obsessive drug cravings, it allows her patients to pull their lives together and learn how to live without drugs.
Clinical studies show that U.S. Food and Drug Administration-approved opioid addiction medicines like buprenorphine offer a far greater chance of recovery than treatments that don’t involve medication, including 12-step programs and residential stays.
But as the country’s opioid epidemic kills more and more Americans, some of the hardest-hit communities across the country don’t have enough doctors who are able — or willing — to supply those medications to the growing number of addicts who need them.
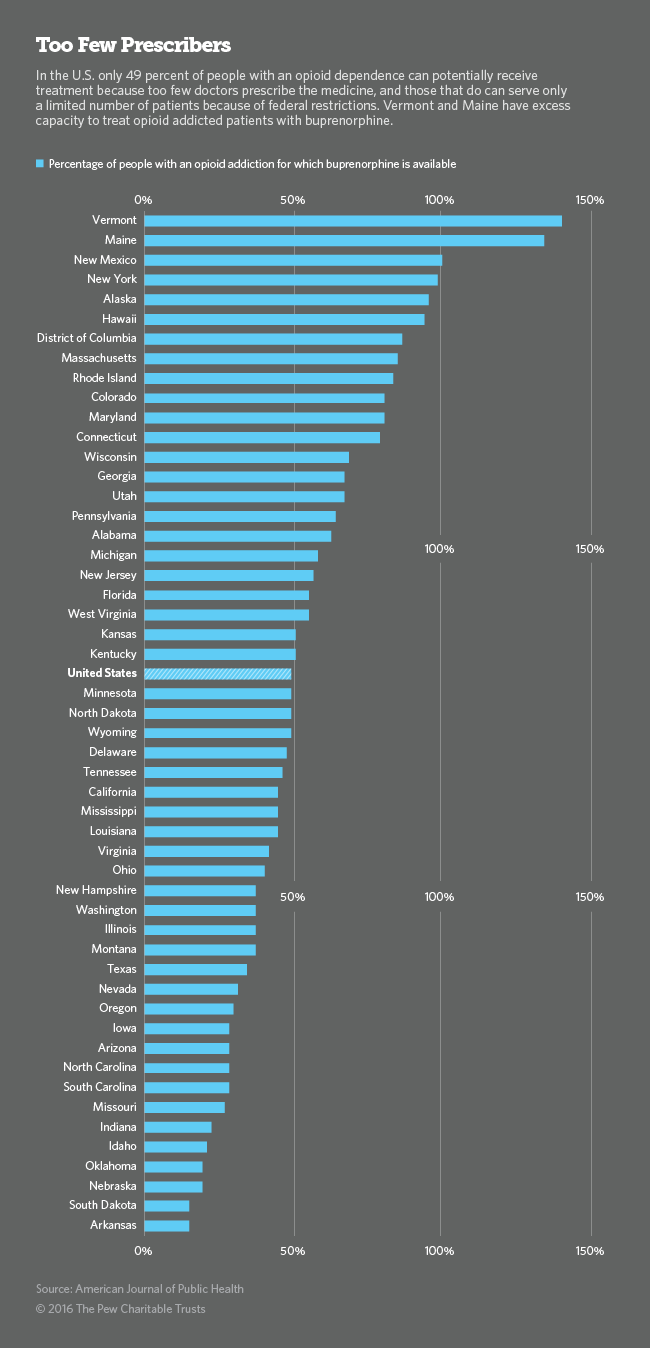
More than 900,000 U.S. physicians can write prescriptions for painkillers such as OxyContin, Percocet and Vicodin. But because of a federal law, fewer than 32,000 doctors are authorized to prescribe buprenorphine to people who become addicted to those and other opioids. Most doctors with a license to prescribe buprenorphine seldom — if ever — use it.
Buprenorphine is the primary addiction treatment tool for Eagen and the seven other staff physicians at the Tom Waddell Urban Health Clinic.
Getting patients started on the medication can be time-consuming. When they’re too busy with other patients, they rely on a small medical team at a county-funded center in the nearby Mission District to screen patients and, if the medication is appropriate for them, determine the correct dose.
At this central “induction center” on Howard Street, a half-time doctor, two nurse practitioners, a behavioral health counselor and two administrators have been providing screening and initial care for low-income opioid and heroin addicts since 2003.
Eagen said working with the Howard Street team makes her life easier. “When the patient is handed back to me, I know that the person is not at risk for imminent relapse. They’re the easiest patients I have.”
Unrealized Potential
With its long history of providing drug treatment and free health care to uninsured residents, San Francisco is particularly well-equipped to battle the opioid and heroin epidemic. But even here, federal prescribing restrictions and lack of information keeps many doctors from entering the fray.
When the National Institute on Drug Abuse funded the research that led to buprenorphine’s development more than a decade ago, it hoped that office-based prescribing of buprenorphine, which comes in a soft tablet and dissolvable film, would mean greater access to addiction medication nationwide.
It hasn’t happened. Most doctors claim they don’t have the training or the time to treat high-maintenance opioid addicts in their busy practices, despite urgent calls from federal and state officials. “I really think doctors are scared of prescribing it,” Eagen said. “They worry they’re going to make people sick when they start taking it.”
But an increasing number of physicians are starting to push for greater use of buprenorphine.
“We doctors are the ones who caused this epidemic by overprescribing pain medications. We need to get more involved in fixing it,” said Kelly Pfeifer, a physician with the California HealthCare Foundation, which advocates for greater availability of addiction treatment and prevention.
Nationwide, about 21.5 million people 12 and older, or 8 percent, had some kind of substance use disorder in the past year, according to a national survey by the U.S. Substance Abuse and Mental Health Services Administration. Of those, almost one in 10 were hooked on painkillers — 1.9 million — and more than half a million were hooked on heroin. And those numbers are rising. Among the low-income adult population served by Medicaid under the Affordable Care Act, the rate is much higher: An estimated 13 percent of newly eligible Medicaid enrollees suffer from addiction.
In California, which was among the first states to expand Medicaid, as many as 370,000, of the 2.9 million people newly eligible for Medicaid, may be in need of treatment.
Under a first-of-its-kind agreement with the federal government, California’s county-run Medicaid programs are slated to begin covering a full set of addiction treatment options recommended by the American Society of Addiction Medicine, including opioid addiction medications. San Francisco County and the rest of the Bay Area will be the first to roll out the new drug treatment benefits later this year.
Federal Rules
Three medications have been approved to treat opioid and heroin addiction. Methadone, a long-acting opioid that fulfills the addicted brain’s perceived need for heroin, was approved for treatment in 1964 and is dispensed at highly regulated clinics scattered around the country, mostly in urban areas.
Patients must visit the clinics daily to swallow a liquid dose of methadone under supervision of a certified health professional. For many, that means traveling substantial distances early in the morning before work. Some patients can qualify for take-home doses for use on weekends.
Naltrexone, a daily pill approved in 1984 for heroin addiction, can also be prescribed by a doctor. But until 2010, when naltrexone was introduced in injectable form, as Vivitrol, it was considered much less effective than either methadone or buprenorphine at keeping people in recovery from heroin addiction.
Buprenorphine, approved in 2002, is prescribed by doctors in an office setting, making it much more convenient than methadone. Patients simply pick up a monthly supply of the medication and take it on their own. Like methadone, it is a long-acting opioid that relieves drug cravings and physical withdrawal symptoms with fewer of the side effects of other opioids.
In anticipation of buprenorphine’s approval, a 2000 federal law required doctors to seek a special license from the U.S. Drug Enforcement Administration to prescribe it. The federal law requires eight hours of training and limits the number of patients per doctor to 30 in the first year and 100 in subsequent years. That limit was established to prevent “pill mills,” in which doctors prescribe the medication for a fee without ensuring that patients are actually using the pills to stay in recovery from a drug addiction.
Although the vast majority of doctors with a buprenorphine license see only a few patients, the federal limit prevents some doctors in high-demand communities and urban neighborhoods from providing care to everyone in need.
In response to the worsening heroin and opioid epidemic, the U.S. Department of Health and Human Services is considering an increase in the patient limit for prescribing buprenorphine. Advocates for greater availability of addiction medicines argue HHS should go further, eliminating the cap altogether and allowing nurse practicioners and physician assistants to prescribe the medication.
But the federal government argues that without adequate record keeping and physician oversight, too many patients could end up selling the medication on the street.
Although buprenorphine does not produce the euphoric effects of heroin, many drug users purchase it to tide themselves over until they can score the real thing. Doctors who advocate for greater use of buprenorphine argue that the threat of diversion is minor compared to the lifesaving potential of the drug.
‘Summer of Love’
Buprenorphine doesn’t just save lives by fighting addiction, advocates say. It also connects drug addicts to mainstream medical care and can help improve their health, which drug users typically neglect.
Dr. David Smith, a San Francisco physician credited with starting the first free health clinic in the country, in 1967, argues that in the long run, patients are better off in the care of physicians than addiction treatment providers, such as counselors and therapists, without medical training.
“We’re finding that when people with addictions start going to a primary care doctor, their physical health starts to improve, too. They start getting regular treatment for diabetes, infections and heart disease, for example,” Smith said. “They tend to stay in treatment longer and their outcomes tend to be much better.”
Smith, who runs a private addiction practice here, treated young middle-class kids who flocked to the Haight-Ashbury neighborhood during the “Summer of Love,” in 1967, to experiment with drugs. Many were dying of overdoses and nearly all of them were neglecting their health, he said.
“I came to a realization back then that health care was a right, not a privilege, and I’ve never changed my thinking,” Smith said. Hundreds of other doctors came to the same realization in the 1980s, when the city became ground zero in the AIDS epidemic.
Then in the 1990s, heroin returned and doctors realized that intravenous drug users were getting HIV. “People were dying all over the city,” said Dr. Judith Martin, medical director for substance abuse services at the San Francisco Department of Public Health.
Many of San Francisco’s doctors began embracing methadone, the only addiction medication back then, Martin said. Addicts who showed up at clinics to get their daily cup of methadone weren’t dying of overdoses and they weren’t contracting AIDS. As a result, Martin said, the department’s doctors are believers in addiction medicines and they’re committed to fighting the disease.
As soon as buprenorphine was approved, the department asked all of its doctors to apply for federal permission to prescribe it, and nearly all did. They were eager to help. But the prospect of fitting droves of drug-addicted new patients into their busy practices worried them.
So in 2003 the department and San Francisco General Hospital teamed up to make it easier for doctors to work with patients fighting addiction. At a cost of about $1 million per year in general tax revenue, more than 1,300 addicts have passed through the Howard Street doors and on to the care of doctors elsewhere in the city.
Once the clinic transfers patients to a primary care provider, they are removed from the rolls, allowing Howard Street’s lone doctor to keep initiating people on buprenorphine without exceeding her 100-patient limit.
San Francisco has seven methadone clinics, more than most cities its size. It also has two mobile clinics that travel to underserved neighborhoods and the jail. Three primary care sites and two pharmacies are also licensed to distribute methadone.
Getting Started
On a rainy Monday morning earlier this month, four of the eight patients in Howard Street’s Spartan waiting area sat uncomfortably on metal chairs looking like they had the flu. They were the ones scheduled to receive their first dose of buprenorphine. A handful of other patients looked much happier. They were the ones who had gotten through the rough part.
For patients who decide to quit opioids or heroin and get on buprenorphine, the first step is to stop using drugs for at least 12 hours or until they start having at least moderate withdrawal symptoms — chills, fever, body aches, watery eyes and restlessness.
That’s what they’re told when they walk in to the center on the ground floor not far from the city’s financial district, in the same building as the Department of Public Health’s mental health and residential substance abuse branch. From the Tenderloin, it’s a short walk downhill.
Patients come on their own to sign up or get referred here by a primary care doctor, a county jail or a hospital. Many want to try buprenorphine but don’t know what to expect. Some are on their second or third try at sobriety.
The first visit takes at least two hours, sometimes more, and patients are almost always filled with anxiety, said Jadine Cehand, the nurse practitioner on duty. Many are ambivalent about their decision to quit, she said. Nearly all patients are fearful of what lies ahead. “We keep telling them that they’re doing the right thing,” she said.
After the first day, patients take a dose or two of the medication home with them and come back every morning for the rest of the week to report their symptoms and get another dose. Check-ins can be less frequent the week after, depending on how they respond to the medication. “It’s amazing to see how quickly they improve,” Cehand said. “By the end of the week they come in with their hair washed and a smile on their faces.”



9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))







{kind=link}