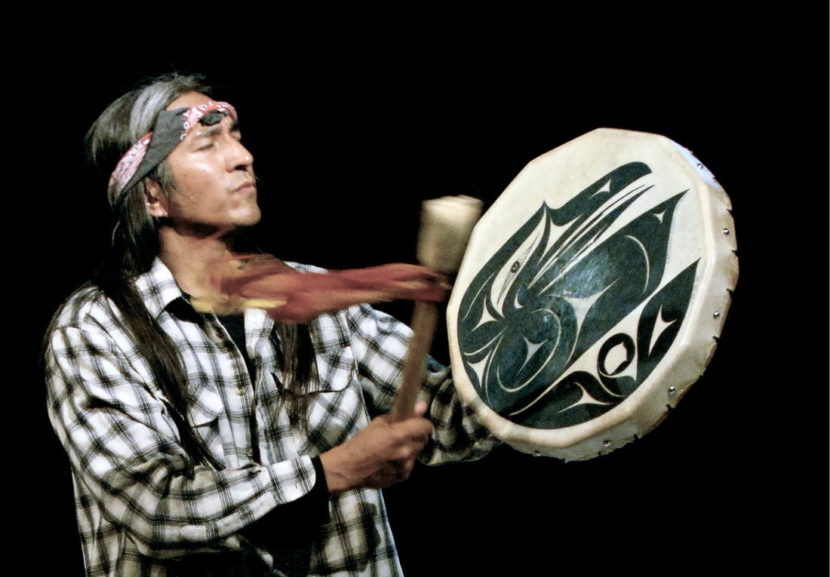
Gene Tagaban helped conduct the Compass training in Dillingham in mid-March. (Photo courtesy of Gene Tagaban)
The Alaska Network on Domestic Violence and Sexual Assault helped organize the training, which was taught by Gene Tagaban, a Tacoma, Washington resident originally from Juneau.
Tagaban said the class is meant to help stop the cycles of violence that are prevalent in many Alaska communities.
“It’s about teaching men to be mentors, and getting men involved to stop the violence, domestic abuse, the suicides, the hurts, the pain,” he said. “For so many years, women have been at the forefront of this movement, of wellness, of health. And as men, we need to be standing right beside the women together, to stop the violence, to stop this epidemic that’s going through Alaska.”
Compass is part of the Alaska Men Choose Respect effort. Participants talked about how to start conversations and lead healthy lives, both in their own homes and in the community.
Tagaban said the group discussed several topics, including respect for self and others, communication and conflict resolution.
“Ultimately, what does it mean to become a man, but even higher than that: what does it mean to become a human being,” he said. “… it’s about learning how to express ourselves in that way and share our stories, tell our stories, learning about where our stories came from. And learning about even, not only our empowerment but the pains, the hurts, the trauma and healing from that. It is about healing. But it’s about men working together to bring that healing together.”
Throughout the gathering, participants shared their own stories and learned how to facilitate those sorts of discussions. After the training, Tagaban hopes they’ll take what they’ve learned back out into the community, whether that’s doing presentations in schools or living a good life and leading by example.
“And I hope that they’ll go out and live a good life, a life of awareness, a life of empowerment, so that in their circles that they can influence those in a good way,” he said. “And maybe some of them will use it to start making presentations, talking about these things, and starting the conversations… that they’ll maybe go to schools and start talking about things, or just in the neighborhoods, in the stores that people would just see them living that powerful life that good life, and then passing it on in their own families, and teaching in their own families, or the schools.”
Used heroin syringes and cooking spoons in a park in Ohio. Some local and state officials are pushing for legal sites where heroin users can inject drugs under medical supervision. AP
A bustling economy. Record-low unemployment. A ballooning heroin problem.
That’s how Mayor Svante Myrick describes Ithaca, New York, where he hopes to open the nation’s first safe injection facility — a place where heroin users could shoot their illegal drugs under medical supervision and without fear of arrest.
His proposal, part of a plan to address drug abuse in the 31,000-person college town in central New York, is not a novel idea. Safe injection sites, which also connect clients to treatment programs and offer emergency care to reverse overdoses, exist in 27 cities in other parts of the world. Some have been around for decades.
But no safe havens for injecting illegal drugs exist in the United States, which is experiencing an epidemic of opioid addiction and a rising tide of overdose deaths. Some lawmakers in California and Maryland want to change that and make legal what addiction specialists say is already going on at many clinics or needle-exchange programs across the country.
Proponents of the sites say they reduce the risk of dying from heroin use because addicts are drawn out from alleys, public restrooms and run-down buildings and into supervised settings where they can be quickly treated for overdose symptoms. Once there, access to clean needles reduces an addict’s exposure to infections, as well as diseases like hepatitis C and AIDS. And, supporters say, drug users are more likely to pursue addiction treatment once they develop trusting relationships with clinic staffers.
Other lawmakers, however, warn that supervised heroin shooting galleries run contrary to state and federal drug laws and would encourage illegal drug abuse.
In New York’s Tompkins County, a jurisdiction of just over 100,000 people that includes Ithaca, at least 14 deaths were drug-related in 2014, up from six in 2010. An addiction treatment center there reported that more than a quarter of its admissions in 2014 were for opioids, second only to alcohol.
“We’re not the capital of heroin in America or even in New York state,” Myrick said. “But we’re losing people.”
Studies of safe injection sites, largely in Canada and Australia, have found that they help reduce overdoses and don’t increase drug use or trafficking in the communities where they’re located.
Sites in the United States could violate the federal Controlled Substances Act, which prohibits possession of drugs such as heroin or cocaine or operating a place where people use them. But Congress could change the law or the U.S. Justice Department could make exceptions for the sites, said Leo Beletsky, a law and health sciences professor at Northeastern University.
Most state laws mirror the federal act and would also need to be amended to allow injection sites to operate legally, he said. Though if states begin legalizing them, the federal government could choose not to prosecute people who run and use them — just as the Justice Department has decided not to enforce federal laws for possessing, processing or selling marijuana in states that have legalized it.
“Do you try to solve these [legal] problems first? Or do you proceed with what you know is needed, the innovation that is needed in, really, a time of national crisis?” Beletsky said.
Advocates would rather establish the injection sites through legislative action, but creating the sites through executive orders issued by mayors or county executives could create quicker access to care, he said.
Even with the approval of the district attorney in Tompkins County, Gwen Wilkinson, Myrick is not interested in opening a site in Ithaca without permission from the New York Legislature and Democratic Gov. Andrew Cuomo.
“Our hope is once this is put in place, we’ll be ready for the next epidemic,” he said.
Legislative Effort
Maryland state Del. Dan Morhaim, an emergency room physician, wants to create safe injection sites in his state, saying supervised injection would help break the cycle of drug use by exposing addicts to counseling and making them less prone to drawing others into the habit of drug use.
Morhaim’s proposal received little opposition during a recent legislative hearing, and officials at the University of Maryland School of Medicine said they would “seriously consider” establishing a pilot program to evaluate the concept if the legislation passes.
“If all our polices were doing great, we’d be talking about how addiction rates are down and streets are safer,” said Morhaim, a Democrat.
Opioid deaths in Maryland increased by 76 percent between 2010 and 2014, to nearly 900. And according to the American Society of Addiction Medicine, drug overdoses are the leading cause of accidental death in the United States. In 2014, heroin contributed to about 10,600 deaths nationwide.
But proposals like Morhaim’s and Myrick’s are not without opposition.
Steve Schuh, a Republican county executive from Anne Arundel County, Maryland, called Morhaim’s bill one of the most “irresponsible” that the General Assembly has ever considered.
Providing those in the throes of addiction a place and the tools to use heroin is “careless, reckless, and unconscionable” and tantamount to making the state an accomplice to murder, he said in a letter to the chairman of the health committee, which held a hearing on the bill this week.
New York state Assemblyman Edward Ra, a Republican, opposes Myrick’s Ithaca plan because he said it would stand in the way of cooperation between local, state and federal law enforcement. The state should instead focus on treating more heroin addicts, Ra said.
“I object to the idea that this drug can be used safely. It’s a drug that kills people.”
Matt Curtis, policy and program director at Voices of Community Activists & Leaders (Vocal), a nonprofit that offers counseling, hepatitis screening, syringe exchanges and other services to drug users in New York City, said it would be easier to establish injection sites locally than at the state level. A campaign for injection sites in New York City already has the support of at least one city councilman.
“We’re not quite there,” Curtis said. “We are still in the stage of getting people familiar with the idea.”
Already Happening
Although no sanctioned injection sites exist, advocates for them say informal sites exist at needle exchanges around the country where addicts can already get clean syringes and substance abuse counseling.
Organizations that operate exchange programs say they do not condone drug use and injection is still prohibited on-site. But because people use bathrooms at the exchanges to shoot up after receiving new needles, the organizations have taken steps to make those spaces safer.
In the past, staff at some exchanges tried to discourage drug use by installing black lights so users couldn’t find their veins and timing how long each person spent in the bathroom. But these practices led to overdoses as drug users rushed to take large amounts of heroin before being detected by staff members.
“That is terrible public health practice and you’re basically saying, ‘Go out and use it in the street,’ ” said Curtis of Vocal, which runs a facility in Brooklyn.
Now, many exchanges have installed syringe disposal boxes, put intercoms in the bathrooms and installed emergency locks so staff members can get into a bathroom to help if someone becomes unresponsive.
Vocal made similar renovations to its facility in 2014, not because very many people were using drugs in the bathroom, Curtis said, but because the changes make the site safer for clients and staff.
Reducing Harm
Supervised injection sites are part of a “harm reduction strategy” to reduce the negative effects of drug abuse through public health initiatives. The harm reduction theory stresses the rights of drug users and acknowledges that abstaining from drug use is not the only measure of improving the quality of life of an addict.
The Boston Health Care for the Homeless Program is applying this theory in its new Supportive Place for Observation and Treatment Center. The center prohibits drug use and won’t offer needle exchange. But users can come there after they inject to wait out their high under medical supervision and there is an exchange close by, said Jessie Gaeta, the group’s chief medical officer.
As many as a handful of clients overdose at the main Health Care for the Homeless site each week and Gaeta said she thinks the rate of overdoses in the Boston area is increasing because people are taking heroin that is combined with other drugs like benzodiazepines, which also have a sedative effect.
“Dead people don’t recover,” Gaeta said. “Our hope is to make it less dangerous for the people who are currently using, who are not seeking treatment or not able to access treatment. I like to think we’re enabling people to live.”
A sign for a Baltimore overdose reversal program. To stem the death toll in the opioid epidemic, cities and states, as well as the federal government, are promoting greater use of the overdose rescue drug naloxone. (The Pew Charitable Trusts)
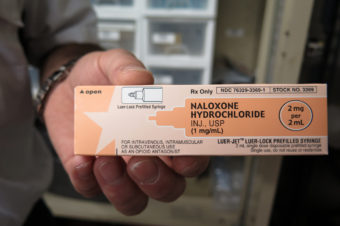
BALTIMORE — A crowd quickly gathers here on one of West Baltimore’s many drug-infested street corners. But it isn’t heroin they’re seeking. It’s a heroin antidote known as naloxone, or Narcan.
Two city health department workers are holding up slim salmon-colored boxes and explaining that the medication inside can be used to stop someone from dying of a heroin overdose. Most onlookers nod solemnly in recognition. They’ve heard about the drug. They want to know more.
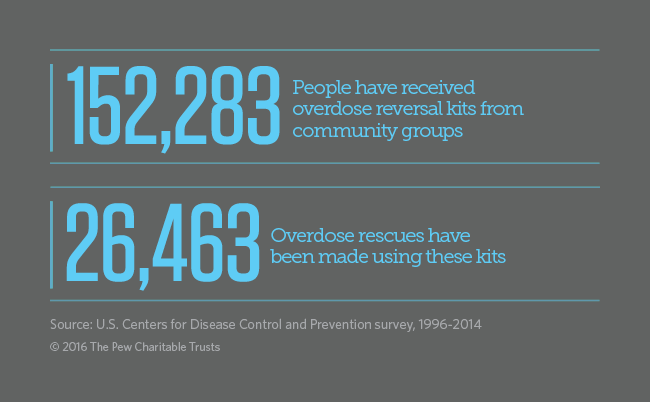
Nationwide, more than 150,000 people received naloxone kits from community outreach programs like Baltimore’s between 1996 and 2014, and more than 26,000 overdoses were reversed using those kits, according to a recent survey funded by the U.S. Centers for Disease Control and Prevention.
In addition, police, emergency medical technicians and emergency room physicians have used the drug to save tens of thousands of lives. Baltimore police officers started carrying the kits last year.
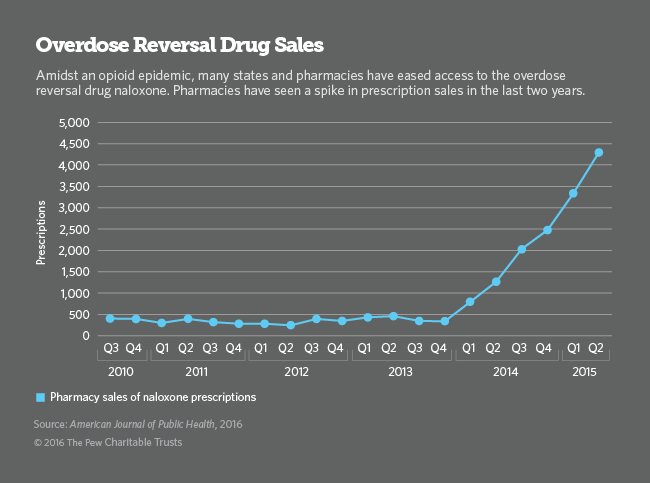
But as the opioid epidemic seeps into nearly every small town and suburb across the country, state, local and federal officials are trying to make the life-saving prescription drug available everywhere, particularly at local pharmacies.
To accomplish that, New Mexico last week became the 29th state to adopt a law that allows doctors and other prescribers to write a naloxone prescription known as a standing order, enabling local pharmacists to distribute the overdose rescue drug to anyone who asks for it.
Maryland adopted a similar measure in October. The day after it took effect, Baltimore’s health commissioner, Dr. Leana Wen, wrote a standing order for the entire city, allowing anyone who completed a simple naloxone training — like the demonstration offered on the West Baltimore corner last week — to walk into a pharmacy, show a certificate of completion, and walk out with a kit.
“I like to say I became the prescriber-in-chief,” Wen said.
New Mexico’s new law updates a 15-year-old law that allowed lay people to administer naloxone. In addition to allowing standing orders, the new measure allows people without a medical license to distribute naloxone kits in their communities, a legal provision found only in Maryland and 12 other states. This exception allows jails, treatment centers, homeless shelters and others to hand out the drug. Even the local PTA could offer it.
“It needs to be in everyone’s first-aid kit and medicine cabinet,” Wen said.
A Nationwide Movement
Forty-two states have enacted laws to make naloxone available beyond hospitals. New Mexico, which has had one of the highest drug overdose rates in the country for more than two decades, was the first to act with its 2001 law.
After more than a decade, Massachusetts in 2012 became the second state to enact a law. Most other states adopted so-called rescue drug measures in 2014 and 2015 after the opioid epidemic began making headlines.
This year, “States are going back and expanding or tweaking their laws,” said Amber Widgery, who tracks these and other drug related laws at the National Conference of State Legislatures.
Thirty states also have adopted so-called good Samaritan measures, which give limited legal immunity to a bystander or friend who calls 911 to report an overdose. Those laws also need to be expanded, said Corey Davis, an attorney who tracks the laws for the Network for Public Health Law.
In Maryland, for example, the law only protects overdose bystanders from being arrested, charged or prosecuted for possession of a controlled substance or use of drug paraphernalia. It does not protect them against arrests for open warrants or probation and parole violations, which are common among heroin and opioid addicts. As a result, residents of West Baltimore or other communities where drug use is prevalent may be unwilling to call 911.
In addition to state and local actions, initiatives at the federal level are picking up. Last week, the U.S. Senate passed a comprehensive opioid addiction and overdose prevention bill that would expand the use of naloxone, and the U.S. Department of Health and Human Services announced additional funding for naloxone and other drug treatment services.
A ‘Miracle’ Drug
The majority of opioid overdose victims die from lack of oxygen one to three hours after they have taken a drug, leaving a substantial amount of time for someone to intervene and administer naloxone or call for help.
Naloxone, approved by the U.S. Food and Drug Administration in 1971 in injectable form and widely used as a nasal spray, is a relatively cheap generic drug that has been proven safe and effective at reversing the deadly lung suppression that can cause a fatal overdose. Once the drug is administered, most victims instantly begin breathing again; they also experience nausea and other withdrawal symptoms.
But until the late 1990s, naloxone was only used, intravenously, in hospital emergency departments and operating rooms. Even emergency medical personnel and other first responders did not use it initially.
In 1996, a community group in Chicago that provided clean needles and other assistance to drug addicts began handing out naloxone as a nasal spray as well. Later, similar pilot programs began cropping up in places like San Francisco and New York.
When people began coming back and reporting that they had saved a life with naloxone and wanted another kit, researchers took notice. Eventually, these and other programs handing out naloxone caught the attention of federal and state officials, said Daniel Raymond, policy director for the Harm Reduction Coalition, which advocates for the greater availability of naloxone and other health care services for drug addicts.
In 2006, Massachusetts began using naloxone in public health and social service centers. Along with New Mexico, it funded statewide distribution of the life-saving medication in communities with large numbers of known drug addicts.
But in other parts of the country, naloxone initiatives were limited and mainly local. Then in 2012, the FDA, along with the National Institutes of Health and the CDC, convened a meeting with state and local officials to discuss ways to expand availability of the drug nationwide. Initially, some objected to making naloxone widely available, arguing that it would simply enable more drug addicts to continue shooting up.
Now that more Americans are dying of heroin and prescription painkiller overdoses than from homicides — roughly 28,000 people in 2014 — that argument rarely comes up. Politicians from both parties vigorously support the use of naloxone. Along with increased access to treatment and safer opioid prescribing, expanding the use of naloxone is among the Obama administration’s top three weapons against the epidemic.
Baltimore’s commitment to naloxone began when the health commissioner, Wen, took office, in January 2015. Since then, the department has distributed nearly 6,000 kits to city residents. In addition, the department launched an online training site, dontdie.org, last month. Wen said she plans to work with local pharmacy chains to make it easier for people to walk in, get trained, and leave with naloxone.
More Work Needed
In February, the pharmacy chain Walgreens announced it had used state standing order authority to make naloxone available without a prescription across New York and would do the same in Indiana and Ohio. Pharmacy chain CVS made a similar commitment in Ohio.
But advocates for greater use of the overdose reversal drug worry that most local drugstores won’t stock the drug or supply it on demand. They also fear that pharmacists won’t allow people to use their insurance plans to pay for it.
According to Davis, the public health law researcher, insurance companies are on board with covering the drug. But, because people with naloxone prescriptions won’t be using the drug on themselves, many pharmacists appear to be worried they won’t get reimbursed for, essentially, a third-party prescription, the claims for which are traditionally rejected by insurance companies.
Baltimore has negotiated a $1 copay with the state Medicaid agency and private insurance companies have generally agreed to cover it, Wen said.
Even in Massachusetts, where standing orders have been allowed for years, not all pharmacies stock the medication and not all pharmacists know about it, according to Dr. Alexander Walley, medical director for the state health department.
“We have the legal pathways but not the implementation experience, yet, to make it as successful as policymakers had hoped,” he said. “We’re in the steep part of the learning curve right now.”
From their folding card table in West Baltimore last week, Daryl Mack and Darryl Burrell handed out 15 naloxone kits in less than a half-hour.
After witnessing friends, family members and strangers die on these streets from overdoses, most onlookers seemed eager to try to prevent at least one fatality.
Speaking one-by-one to each person who wanted a kit, Mack emptied the contents of a box onto the table and quickly demonstrated how to assemble and activate the tiny nasal atomizer used to squirt naloxone into an overdose victim’s nostrils.
You’re not going to harm someone who’s unconscious by giving them naloxone, he told them. And you can’t give them too much. But first, try to make sure they’re not just sleeping or passed out from alcohol, Mack said. Rub your knuckles up and down their chest bone to try to wake them up. If that doesn’t work, they need help, he said.
Maryland is the only state that requires anyone using naloxone to complete a brief training, Davis said. Several people who approached the table already knew the drill and were there to get refills. They also got a copy of Wen’s standing order so they could pick up additional kits at their local drugstore if needed.
One passerby heard the word “heroin” and waved the health workers away, saying, “I don’t have nothing to do with that stuff.” But when Mack explained that he could save someone’s life, the elderly man stopped and signed up.
Like many small towns, Kutztown, Pa., is trying to figure out how to steer residents away from heroin. Melissa Block/NPR
The epidemic of opioid abuse that’s swept the U.S. has left virtually no community unscathed, from big cities to tiny towns.
In fact, drug overdose is now the leading cause of injury death in this country: more than gun deaths; more than car crashes.
There were more than 47,000 drug overdose deaths in the U.S. in 2014, according to the Centers for Disease Control and Prevention. That includes unintentional overdoses and suicides. More than half of those were from opioids, including painkillers and heroin.
I went to rural Berks County in southeast Pennsylvania to hear what the opioid epidemic means in a small town, a place where everyone knows everyone and the ripples of addiction spread wide.
Really, I could have gone just about anywhere. No community is immune.
The landscape in Berks County is bucolic: rolling farmland studded with silos and 19th-century stone barns. But that peaceful landscape belies a serious problem. Opioid addiction is deeply embedded in these small towns.
“It’s become a crisis,” says Phil Salamone, a paramedia in Kutztown, Pa.
He points out that heroin is both cheap and readily available from nearby cities such as Reading and Philadelphia. Salamone says, “There is no exclusive demographic that’s using it. It’s everybody. It’s kids, adults, low income, high income. It’s everywhere.”
Paramedic Phil Salamone carries naloxone, a drug used to reverse an opioid overdose. Melissa Block/NPR
Local paramedics have been able to save lives by using the drug naloxone, also known as Narcan. It reverses an overdose by latching onto receptors in the brain and kicking the opiates off.
“We don’t ever have to worry about that medication expiring because it’s always used, Salamone says, somewhat ruefully.
The Kutztown ambulance squad has “Narcanned” ten overdose victims so far this year. Salamone says the drug makes paramedics like him look really good. “You have a patient that is unresponsive. We start an IV on them, administer naloxone and they wake up! Just like nothing had happened.”
Early one morning last May, a neighboring ambulance squad got an emergency call from Brandywine Heights High School. A girl had been nodding off at her desk. She soon collapsed, semiconscious and turning gray. She had overdosed on heroin.
School guidance counselor David Favata, a certified EMS worker, raced in and got the girl breathing with a bag mask. An ambulance whisked her to the hospital and she did survive, but it was a close call.
It turned out she had done heroin in the school bathroom before class that morning.
School principal Josh Ziatyk recalls her as a great kid, a former cheerleader, with “tons of energy and the world ahead of her.” But, he says, “Through the late middle school years into early high school years, there was a change that occurred within her. And little by little, [she] just found herself into a black hole, into a rut, and couldn’t get out of it.”
The opioid epidemic has galvanized Brandywine Heights and neighboring Kutztown Area High School into action. Between them, they lost six former students to heroin overdose within two years.
Students walk the halls in a Kutztown area high school. Melissa Block/NPR
Nurses at the middle and high schools now stock naloxone in the event of an overdose.
Both communities have organized groups to spread awareness about opioid abuse and try to prevent it. They sponsor activities to keep young people engaged. Boredom is a problem in a small town, and drugs can easily fill that void.
At Kutztown High, students meet each week as part of a group called Kutztown Strong, which was formed in response to the drug crisis. When I visit, they’re busy planning a three-on-three basketball tournament.
After the meeting, freshman Ramsi Ross tells me how angry she gets when she reads social media posts about the overdose deaths of young people. “Everyone’s saying like ‘rest in peace, you’ll be missed,’ and I just couldn’t help but think, these were your friends! Couldn’t you have done something? Maybe you should have got involved in Kutztown Strong and stopped your friends from using.”
Of 450 students at Kutztown High, there are about five who are back in school after rehab. And there are quite a few others the staff is concerned about.
Teachers and counselors meet each week with a specialist who has a contract to work in the school. This student assistance team is part of a state-mandated program in Pennsylvania.
They’re on the lookout for kids in trouble. It could be eating disorders, anxiety, self-harm, or drug and alcohol abuse. They look for possible warning signs: kids whose grades have tanked or who’ve changed friend groups.
On the state level, it’s hard to get solid data on whether these interventions are effective. But the staff members at Kutztown High say they’re providing a crucial support network for kids at risk.
Guidance counselor Andrew Brett works at Kutztown High. He says he has seen students migrate from pot to prescription painkillers to, sometimes, heroin. Melissa Block/NPR
Guidance counselor Andrew Brett has seen a recent pattern: kids who start with pot may pivot to prescription painkillers and sometimes — across the spectrum, from the highest achievers on down — to heroin.
“Kids aren’t afraid of it,” he tells me. “Years ago, it was,’Well, heroin is for junkies.’ And you had to be pretty low, and that was the perception. Well, that’s not the perception. It’s available and it’s cheap. And it’s readily available in our community.”
When the student assistance team wants to intervene, they approach the student’s parents first.
School superintendent Kathy Metrick says that conversation doesn’t always go so well: “I sat across the table from a parent whose child had been found in possession of all sorts of paraphernalia, and she said he was picking up trash off the street, that he would never do that.”
Metrick goes on, “The denial is just so powerful. And you want to say, ‘Please save your child!’ Because, if we’re wrong, yay! That would be the best news ever. But gosh, if we’re right and we have a chance to step in now before it’s too late, let’s do that.”
But Metrick knows even if they do step in, that’s no guarantee.
Students will likely come back from rehab to the same circle of friends, the same triggers and temptations as before.
Copyright 2016 NPR. To see more, visit http://www.npr.org/.
James Gallanos is a prevention program coordinator with the Alaska Department of Health and Social Services’ Division of Behavioral Health.
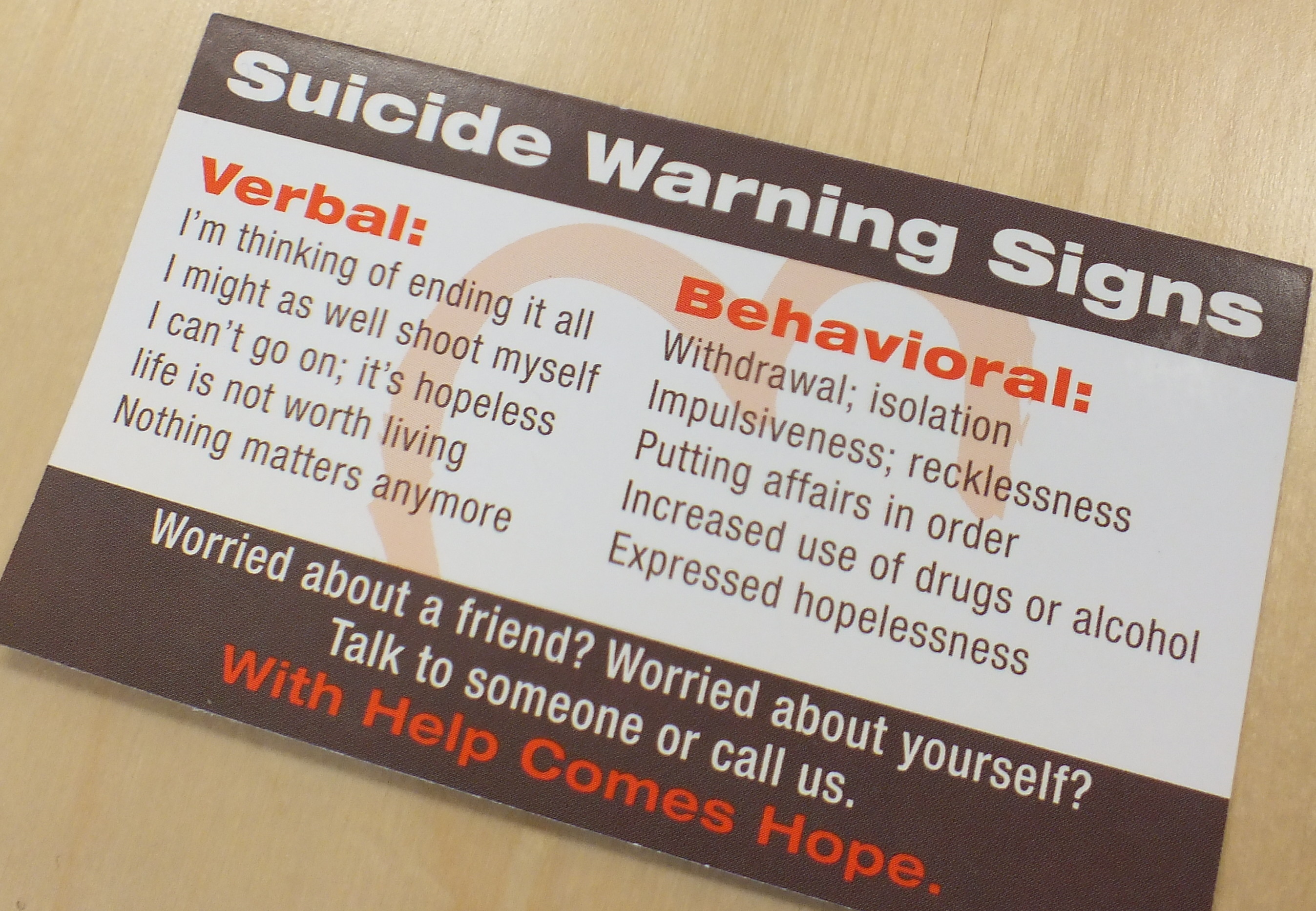
In an interview that aired in three parts on KTOO’s Morning Edition program, Gallanos talked about the Careline Alaska, safe messaging by the media during coverage of a public suicide, how to talk or comfort those who may have witnessed a suicide, and what to listen for if a family member or friend is contemplating suicide.
Safe messaging
Gallanos said safe messaging by the media includes avoiding images which show the method or location of a suicide.
“How can we cover a story while, at the same time, use words and phrases that are less harmful, more hopeful and helpful for people affected by the loss,” Gallanos said.
Listen to part one of the interview about safe messaging:
Making sense of suicide
Gallanos said it’s not uncommon for everyone to experience some degree of shock while responding to a suicide.
“The biggest question we have around suicide is ‘Why? Why would someone take their life?'” Gallanos said. “That makes it difficult because that’s why suicide is such a profound loss. We don’t always have the answers to why someone takes their life.”
Listen to part two of the interview about talking to witnesses of a suicide:
(Since this interview with Gallanos on Tuesday, KTOO was able to determine that a group of children believed to be in the vicinity of the Dimond Courthouse during Monday morning’s incident was too far away to actually see what had happened.)
(Photo by Matt Miller/KTOO)
“Nobody cares about me. I won’t be around any longer to worry about it.”
Gallanos said many of those contemplating suicide are unlikely to say it directly, and many of the indications will come in coded language or messages.
“Maybe it’s important that I invite the question about if they’re experiencing suicidal thoughts or thinking about killing themselves,” Gallanos said. “Very difficult question to ask, but very critical and important question to ask.”
Listen to part three of the interview about talking to those who may be contemplating suicide:
The House Finance Committee sent its budget proposal to the full House of Representatives on Wednesday. The budget, with some late changes, would cut spending by $280 million. It also spends $225 million in funds left from the current budget.
There were some intense exchanges between committee members before the final vote.
Rep. Lynn Gattis, R-Wasilla, during discussions about the state operating budget shortly before it was passed out of the House Finance Committee, March 9, 2016. (Photo by Skip Gray/360 North)
Wasilla Republican Rep. Lynn Gattis questioned why the leftover funds from the current budget only emerged recently.
“Folks in my district are saying, ‘Why in the heck would I trust you to go and tax me or take my Permanent Fund dividend, when you guys are playing these shell games?’” she said.
But Eagle River Republican Rep. Dan Saddler said spending the savings was a legitimate budget strategy.
On Tuesday, the committee added $30 million for an addiction treatment program, and restored $2.7 million for public broadcasting and $1.7 million dollars for the Nome Youth Facility.
Anchorage Democratic Rep. Les Gara said the budget shortchanged vulnerable Alaskans. He noted the spending plan cuts all state funding for pre-kindergarten.
Rep. Les Gara, D-Anchorage, during discussions about the state operating budget shortly before the House Finance Committee passed it on Wednesday. (Photo by Skip Gray/360 North)
“I understand we have to cut waste. But we don’t have to cut the things that make a difference in people’s lives,” he said. “That’s where I draw the line. And we crossed that line over and over and over yesterday. I don’t believe we have to cut things that senior citizens rely on. Three hundred and fifty thousand dollars got cut from senior citizen help for people who need emergency housing.”
But Committee Co-Chairman Mark Neuman said that as the state considers cutting Permanent Fund dividends and raising taxes, it must cut spending.
“I’ve had to tell every group, every person that’s walked into my office that has approached me on the street – wherever they talk to me – no. I can tell you, look you straight into the eye that everybody that has walked into my office was told no, we don’t have the money.”
The House is scheduled to discuss the budget — and potentially vote on it — on Thursday. The Senate may vote on its version of the budget on Saturday. Then the two houses will work to resolve the differences.
Close
Update notification options
Subscribe to notifications
Subscribe
Get notifications about news related to the topics you care about. You can unsubscribe anytime.






9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))