Fish drying in the village of Togiak. (Public Domain photo by U.S. Fish and Wildlife Service)
The Togiak traditional council has rolled out the “not welcome” mat to a Dillingham man they say has been importing alcohol and drugs into the community.
This is the second time in a year that the Togiak tribe has banished an individual from the village. Last fall, local air carriers were informed that the first of them, a 23-year-old from Dillingham, was no longer welcome in Togiak. On Friday letters went out that the second had been banished as well. He, a brother to the first, is 26 years old.
“I think we need to do this, to protect our future children, and our elders, because they’re vulnerable. It’s been getting worse, and we’re saying enough is enough,” said traditional council president Jimmy Coopchiak.
The tribe has decided not to publicly release the men’s names. Because the allegations of drug and alcohol importation leveled against the men are not based on state criminal complaints or filed in open court, KDLG has withheld their names from this report.
Local airlines confirmed that the tribe had asked them not to allow either of these brothers passage to the village.
Banishments from tribal lands in Alaska are not necessarily common but are not unheard of. The procedure appears to be of renewed interest as communities wrestle with the epidemic of heroin and meth use.
“It’s rare, but we are exercising our sovereign authority as a federally-recognized tribe,” said Togiak tribal court clerk Helen Gregorio.
Gregorio said banishment begins with a petition to the tribal council, which then meets with the court’s three-judge panel. Once the banishment order has been signed, the tribe says its police force will arrest the men if they set foot on their tribal lands.
The first man was banished for life, the most recently banished for the next 10 years.
Coopchiak said the council is taking more petitioned cases under consideration right now, these involving actual tribal members who live in Togiak.
“If it’s a tribal member, we have the authority to revoke their membership in our tribal membership,” he said.
Coopchiak and other officials in Togiak, a dry village, say the amount of hard drugs and alcohol coming in has spiked dramatically in the past two years. They blame that in part on direct cargo flights from Anchorage, and a lack of enforcement. They say they are asking the state and federal governments for help, hoping for funding and expanded jurisdiction for their tribal police and court.
First lady Donna Walker and Gov. Bill Walker talk to a man at Saturday’s Hope, Not Heroin event. (Photo by Elizabeth Jenkins/KTOO)
The Juneau Police Department recently held an event to bring people and service providers together called Hope, Not Heroin. Alaska lawmakers were there, as well as Gov. Bill Walker. And for some in the crowd, the event signified how communities are changing the conversation when it comes to talking about addiction.
Hope, Not Heroin started off with a Juneau firefighter describing how he uses Naloxone, also known as Narcan, in the field.
“Giving Narcan, we want to make sure that they are actually overdosing on an opiate,” he told the crowd.
It’s an emergency drug that can save a person dying of an overdose. And it won’t be just emergency responders administering it anymore. Since the legislature passed Senate Bill 23, some Alaska pharmacies could start carrying it as early as the summer. Family members or friends could have access to the drug.
That’s one of the reasons why 19 year-old Nichelle Williams said she wanted to be here: Naloxone saved her life.
“I just came out of treatment from a heroin overdose. And so I came here to help support the bill and everything that’s going on with the heroin stuff,” Williams said.
Williams is exactly who this event is for. Around the room, there are about 31 booths with information about addiction, recovery, even proper syringe disposal. But for such a heavy topic, the atmosphere is light. There’s folky music and a food truck selling pizza.
Rick Hanby is sitting around a table with his wife and kids. He said they decided to come because they’ve known someone who’s struggled with opiate use.
“I think sooner or later, or one way or another, it affects somebody, everybody here. It affects our community. So this is a really good start to get everyone to start thinking and start talking about it,” Hanby said.
Lt. Kris Sell said it’s not common for police departments to organize an event like this. But over the past six months, they’ve tried to use other tactics to reduce heroin use. For decades, she said police across the country focused on the narcotics supply in the War on Drugs.
“And so now we’re acknowledging that it’s the demand that fuels this problem,” Sell said.
Event goers watch the governor’s speech at Hope, Not Heroin. Sen. Johnny Ellis, who helped craft SB 23, also attended. (Photo by Elizabeth Jenkins/KTOO)
Seven people died in heroin-related deaths in 2015. This year, there’s been one. And Sell thinks, overall, 200 people in Juneau use heroin on a daily basis.
“Doubling to about 400 during the summer when we get in highly paid seasonal workers, like in the fishing industry. Some of the tourist industry,” Sell said.
So, for those struggling with addiction who want to get help, she said it can be difficult to navigate what treatment options are available. Unfortunately, in Juneau, the answer is not a lot.
Mitzi Privett, the interim director at Rainforest Recovery Center, said typically, they have some beds available for in-patient detox.
“Recently, we’ve been very full,” Privett said. “And so if someone came in that needed help right away, it would be much harder to serve them. If we had more options, we could say, ‘We’re not available to help but let us refer you to somebody who is.’”
Nichelle Williams was one of the people who was able to get in after her heroin overdose. But she thinks Juneau should have more options. Recently, her friend overdosed and died before she could get help.
“And it was really hard, and she didn’t have the option of treatment because when she went into the hospital, they were like, ‘We can’t help you,'” Williams said. “That’s how most people die in Juneau, if they want help and they try to get help, the hospital can’t help them detox.”
With her recovery, Williams said seeing support — like Saturday’s event — has been huge. But there’s still room for growth when it comes to educating people about addiction.
“When people call me a junkie or something, it makes me feel degraded,” Williams said. “I’m a normal human being. I just have an issue. Just the labeling, it really gets people down. It really does.”
While Juneau waits for more addiction treatment, Williams said there’s something else the community can do to help: be positive and keep the conversation going.
Last month, Centers for Disease Control and Prevention called for physicians to consider alternatives to opioids first when treating pain. St. Joseph’s Regional Medical Center in Paterson, N.J., is one hospital implementing an opiod-alternative program. Hansi Lo Wang/NPR
There’s a new tool for battling the opioid epidemic, compressed inside long, metal tanks at an emergency room in Paterson, N.J.
It’s laughing gas, also known as nitrous oxide.
If you think this is a joke, spend a few hours with Alexis LaPietra, medical director of pain management at St. Joseph’s Regional Medical Center’s emergency department. She’s developed an opioid-alternative program that’s trying out unusual ways to help patients through their pain without using prescription painkillers in the ER, where the road to addiction began for many patients.
“What we’ve been doing before didn’t have the best results,” LaPietra says. “Let’s try a different way besides pills, which I know are easy to take. But they have risks.”
Risks of overdose and sometimes death drove the Centers for Disease Control and Prevention to put out national guidelines in March, calling for physicians to consider alternatives to opioids first when treating pain.
“We are really trying to move outside the box because we don’t want our patients to suffer. We cannot allow this to continue,” she says.
To relieve fractures, St. Joseph’s ER now uses ultrasound to find nerves that can be injected with a numbing agent to block the pain. LaPietra says she’s also encouraging patients to try treatments such as acupuncture after they’re discharged from the hospital.
Dr. Jeanmarie Perrone, a professor of emergency medicine at the University of Pennsylvania, studies how emergency departments prescribe opioids. She says this opioid-alternative program is a step in the right direction as other hospitals have tried similar efforts at a smaller scale to cut back on opioids.
“This requires a balancing act,” Perrone says. “This is the art of medicine. This is the appropriate use of our judgment.”
She warns, though, that this shift goes against a longstanding culture amongst many physicians.
“All we’ve really been told is, ‘Make sure that you’ve treated pain adequately so that the patient thinks that their pain is well-controlled,’ and that that translates into treating them with an opioid and as much as they want.”
Perrone says hospitals that try opioid-alternative programs in their ERs may risk getting more negative patients reviews about how they manage pain.
“The point here is not to be for or against opioids any more than it makes sense to be for or against antibiotics,” says John Markman, a neurologist at the University of Rochester who specializes in pain management.
He says any ER’s pain management program still has to keep opioids as an option.
“The goal is to learn to use them skillfully to minimize the public health risks because the public health risks are significant,” says Markman, who’s conducted research on opioids, some of which was funded by pharmaceutical companies. “There are many patients in the right context and in the right hands who can benefit.”
That’s a reality for some cancer patients and other people with severe pain that Mark Rosenberg, chairman of St. Joseph’s emergency department, acknowledges.
“We are not opioid-free,” he explains. “Even though it’s alternatives first, we will use whatever pain medication we need to improve the care of the patient.”
Among the 300 patients from the first two months of St. Joseph’s program, Rosenberg says 75 percent left the ER without needing opioids.
Copyright 2016 NPR. To see more, visit http://www.npr.org/.
Makenzee Kennedy is groomed by nurse Megan Kelly in a special unit for weaning newborns off heroin and other opioids at North Baltimore’s Mount Washington Pediatric Hospital. The number of newborns suffering from opioid withdrawal symptoms has skyrocketed in the last five years. Getty Images
BOSTON — As soon as the home pregnancy test strip turned blue, Susan Bellone packed a few things and headed straight for Boston Medical Center’s emergency room. She’d been using heroin and knew she needed medical help to protect her baby.
“I felt so guilty. I still do,” said Bellone, a petite, energetic woman. At 32, and six years into her heroin addiction, having a baby was the last thing on her mind. “I was not in the right place to start a family,” she said. “But once it was happening, it was happening, so I couldn’t turn back.”
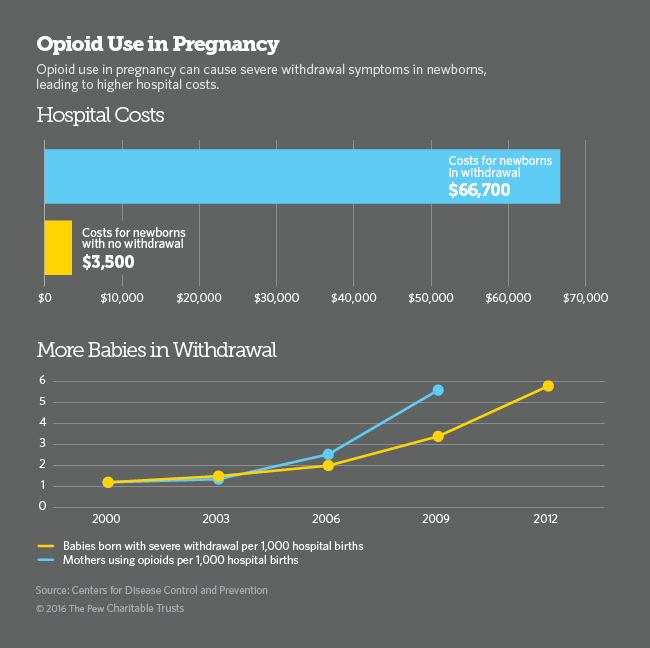
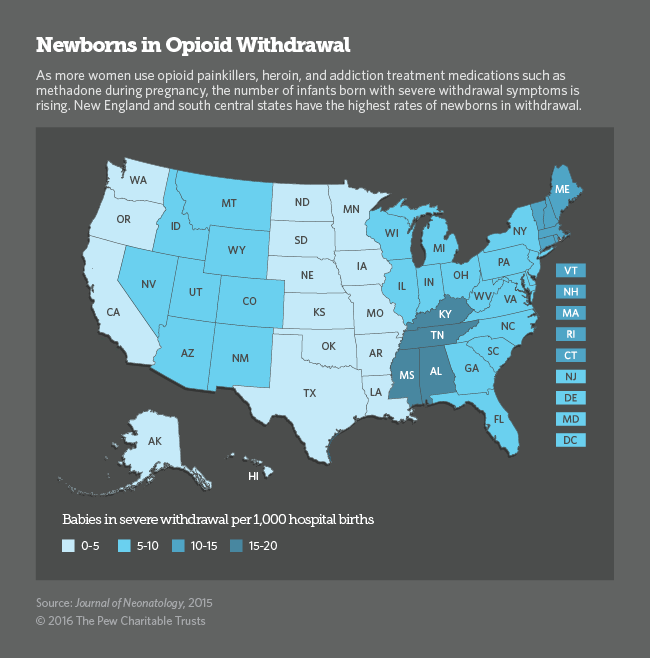
Nationwide, the number of pregnant women using heroin, prescription opioids or medications used to treat opioid addiction has increased more than five-fold and it’s expected to keep rising. With increased opioid and heroin use, the number of babies born with severe opioid withdrawal symptoms has also spiraled, leaving hospitals scrambling to find better ways to care for the burgeoning population of mothers and newborns.
Among the most important principles is that expectant mothers who are addicts should not try to quit cold turkey because doing so could cause a miscarriage. Trying to quit opioids without the help of medications also presents a high risk of relapse and fatal overdose.
Until the opioid epidemic took hold about eight years ago, most hospitals saw only one or two cases a year of what is known as neonatal abstinence syndrome. Now, a baby is born suffering from opioid withdrawal every 25 minutes in the U.S., according to the National Institute on Drug Abuse.
When a pregnant woman uses drugs or alcohol during pregnancy, some of the substances travel through the placenta to the baby. In many, but not all, cases, exposure to opioids during pregnancy can cause the fetus to develop physical drug dependence. When the umbilical cord is cut at birth, the newborn is abruptly disconnected from its supply of opioids and can suffer withdrawal symptoms.
When Bellone rushed to the emergency room six years ago, she didn’t know she’d gone to one of the best places in the country to receive addiction treatment during pregnancy.
At Boston Medical Center in the city’s South End, heroin addiction during pregnancy is not new. A specialized team of obstetricians, addiction medicine providers and counselors known as Project RESPECT has been treating pregnant drug users here for more than 30 years.
Now, dozens of hospitals and health clinics are gearing up to provide the same kind of specialized treatment for a rapidly rising number of pregnant drug users and their newborns
Although painful, newborn withdrawal symptoms, which include muscle cramps, tremors, diarrhea, vomiting, sleep problems and sometimes seizures, are not life threatening and have not been shown to cause health problems or developmental deficiencies later in life. The condition can be treated with small doses of morphine and subsides within a one to three weeks.
Methadone and Buprenorphine
As an epidemic of opioid and heroin addiction continues to ravage the nation, affecting at least 2.5 million people, hospitals and obstetrical practices nationwide have begun collaborating with addiction specialists to find the best way to treat women for their addiction while providing the safest care for their babies.
“Addiction specialists are terrified of treating anyone with a baby inside, and obstetricians are terrified of getting into addiction medicine,” said Dr. Ronald Iverson, of the Massachusetts Perinatal Quality Collaborative. But as demand for prenatal care for opioid-dependent women skyrockets, hospitals and private practices are increasingly offering combined addiction treatment and obstetrical services, so that pregnant women can see both specialists in one appointment.
Last year, a federal law was enacted — the Protecting Our Infants Act — authorizing the U.S. Centers for Disease Control and Prevention (CDC) to work with states to collect data on the prevalence of babies born with opioids in their bloodstream. It also calls on the U.S. Department of Health and Human Services to develop recommendations for the best way to prevent and treat drug use during pregnancy.
The standard of care for pregnant women using prescription painkillers or heroin is maintenance treatment with opioid addiction medications methadone or buprenorphine. Abstaining from drugs without medication is not recommended because of the high risk to the mother of relapse and overdose.
Although methadone and buprenorphine expose the fetus to low doses of opioids, the risk to the newborn of withdrawal symptoms is far outweighed by the risk of a fatal overdose when pregnant women receive no treatment or attempt to abstain from drugs without medication.
Abruptly quitting opioids in the first and third trimesters of pregnancy can cause harm to the fetus, including miscarriage and stillbirth, and is not recommended. Even in the second trimester, specialists agree that the risk of relapse outweighs any potential benefit to the fetus of lowering the dose of addiction maintenance medications or discontinuing their use.
Advocates for newborns, including the March of Dimes, agree with major medical organizations on the use of opioid treatment medication. But they argue more data and better research are needed to determine the best approach to treating opioid addiction during pregnancy.
“With pregnant moms, we’re weighing the high risk of death from overdose against the risk to the newborn of treating pregnant women with low dose opioid maintenance,” said Dr. Siobhan Dolan, medical adviser to the March of Dimes. With more research, she said, “we would be in a better position to consider abstinence and behavioral health counseling for some women.” And that could result in healthier babies.
According to the most recent data from the CDC, the number of opioid and heroin overdose deaths shot up by 14 percent between 2013 and 2014, killing more than 28,000 people, more than 10,000 of whom were women.
Fear and Misinformation
Most women who come into Boston Medical Center for drug treatment and prenatal care do so early in their pregnancy, said Dr. Kelley Saia, who heads Project RESPECT’s team that now treats about 250 patients at any given time, triple the number it did 10 years ago.
“They are so smart and so tuned into what they’re going through,” Saia said. “But they feel incredible guilt about taking medication during pregnancy and they worry about what their babies will go through.”
When Bellone arrived at Boston Medical she was ready to quit heroin. She’d done it before. “I wanted to stop everything. I didn’t even want to be on Subutex [a form of buprenorphine], but they said I might miscarry.”
On top of the normal worries about going through a pregnancy and becoming a parent, women with a drug habit worry about getting reported to child protective services. Massachusetts requires hospitals to report all babies born with opioids in their bloodstream to the state’s child welfare agency.
In many other states, doctors are required to report their patients to child welfare agencies before their babies are born, said Farah Diaz-Tello, an attorney with National Advocates for Pregnant Women, which advocates for the civil rights of drug-using women. In three states — Alabama, South Carolina and Tennessee — women can be prosecuted for child endangerment if they are reported using drugs during pregnancy. (The Tennessee law will not be in effect after July 1.)
Diaz-Tello and others say this threatens the health of women and their babies. Women need to feel safe so they don’t have to hide their drug use when seeking prenatal care or not seek care at all, she said.
Bellone said she wasn’t concerned about getting reported to child protective services because she knew she was doing the right thing. “If I wasn’t ready to quit I would have been worried,” she said. “But I knew five years before I got pregnant that I didn’t want to lead that life. I needed help and didn’t know where to go.
“It was almost like it took me getting pregnant to find help. It was hard to get into any place. There were no beds. But once you got pregnant it was instant, people were willing to help.”
Bellone’s pregnancy and her addiction treatment went smoothly. She delivered twin girls, Gemma and Mischa, on Aug. 3, 2010. They had to stay in the hospital for three weeks, but they’ve been healthy since they came home.
Perched on her chair sipping a huge to-go cup of iced tea in one of the hospital’s private consultation rooms, Bellone passed around photos of the twins jumping on their bed. Gemma, the oldest by seven minutes, just lost a tooth. “She pulled it out herself. She was very brave,” Bellone said.
Nearly six years after their birth, Bellone is still in recovery. She’s taking buprenorphine, making monthly visits to her addiction doctor and attending group meetings two times a week. She’s also working full time as a cook at a nursing home. “I’m tired a lot, like anyone with twins would be,” Bellone said. “People think I’m lying, but I never think about using.”
The Juneau Police Department is hosting an event Saturday to help heroin users and those who have lost someone to the drug. Hope, Not Heroin will have food, music and 31 booths with information about addiction and recovery.
Lt. Kris Sell said it’s not common for police departments to organize an event like this.
“No, and we recognize that fact that we need to do something differently because our old tactics don’t work. The old tactics of just focusing on the supply don’t work, so we have to go after the demand,” she said.
Sell said seven people in Juneau died of heroin-related deaths in 2015. There’s been one death this year, and Sell said the police and fire department haven’t had a call since the beginning of March. Still, she said that number tends to increase in the summer.
To connect people with services, Sell said active opiate users are invited to attend the event.
“They are absolutely welcome, and we’re not going to be patting them down. That’s not what this is about. What we want is for them to get information and see what’s out there,” she said.
Hope, Not Heroin will also have several resources for the family and friends of those struggling with addiction. There will be a memorial wall to commemorate loved ones.
Sell said Capital City Fire/Rescue will be there to give information about Naloxone, which can save someone who’s overdosing. Recently, the legislature passed a bill that makes it easier for pharmacist to dispense Naloxone and gives protections to people administering it.
“They’re are probably going have questions like, ‘Do I tell the addict in my family I have this? Will that encourage brinkmanship in using too much of the drug? Trying to get higher and higher and thinking this is a safety net.’ Those are very real decisions that have to be made,” Sell said.
Hope, Not Heroin is on Saturday from 2 to 6 p.m. at the Juneau Arts and Culture Center. Capital City Fire/Rescue will discuss Naloxone at 2:30.
Doctors are trying to slowly wean Lexi from her dependence on methadone. She’s just 2 weeks old. Under a doctor’s advice, her mom took methadone while pregnant, to help kick a heroin habit. (Photo by Kristin Espeland Gourlay/RIPR)
This story is first in our four-part series Treating the Tiniest Opioid Patients, a collaboration produced by NPR’s National & Science Desks, local member stations and Kaiser Health News.
Swaddled in soft hospital blankets, Lexi is 2 weeks old and weighs 6 pounds. She’s been at Women and Infants Hospital in Providence, R.I., since she was born, and is experiencing symptoms of opioid withdrawal. Her mother took methadone to wean herself from heroin when she got pregnant, just as doctors advised. But now the hospital team has to wean newborn Lexi from the methadone.
As rates of opioid addiction have continued to climb in the U.S., the number of babies born with neonatal abstinence syndrome has gone up, too — by five-fold from 2000 to 2012, according to the National Institute of Drug Abuse.
It can be a painful way to enter the world, abruptly cut off from the powerful drug in the mother’s system. The baby is usually born with some level of circulating opioids. As drug levels decline in the first 72 hours, various withdrawal symptoms may appear — such as trembling, vomiting, diarrhea or seizures.
At some point, if symptoms mount in number or severity, doctors will begin giving medication to help ease them. The idea is to give the baby just enough opioid to reduce those symptoms, and then slowly, over days or weeks, decrease that dose to zero.
A doctor comes to check on Lexi and her mother, Carrie. To protect her family’s privacy, Carrie asked us not to use the family name.
“So, hi, Peanut!” the doctor says to the baby. “Any concerns?” she asks Carrie.
“Coming down has been catching up with her,” says Carrie.
“Do you feel like she’s jittery?” the doctor asks.
“She didn’t want to be put down last night — like [she had] the shakes,” Carrie says.
Lexi has neonatal abstinence syndrome, and has been getting methadone treatments for it. She is getting better — most babies do — but even with treatment, she’s had tremors, diarrhea, and she’s cried and cried. Her little arms and legs tighten up, her fingers and toes clenched. She’s been feverish, her mother says.
“I know what she’s feeling,” Carrie says. “And that is the worst part.”
Carrie was addicted to heroin herself and knows withdrawal is miserable. She’s been off heroin — with help from methadone — since she found out she was pregnant, she says. The small dose of methadone keeps a low level of opioid in her system so she doesn’t go into withdrawal, but it doesn’t get her high. For Carrie and thousands like her, methadone is a lifesaver — helping them quit a heroin or oxycodone or other opioid habit for good.
But getting pregnant posed a dilemma: If Carrie stopped taking opioids altogether, she risked relapse or miscarriage. Yet, if she continued to take any opioid — including methadone — there would be a 60 to 80 percent chance that her baby would be born with neonatal abstinence syndrome, the doctors told her.
“It’s hard to watch, as her mother,” Carrie says, “because you’re helpless and there’s really nothing you can do. You are a lot of the reason why she’s going through what she’s going through.”
Babies going through withdrawal spend weeks — even months — in hospital nurseries like this one.
“Their cry is very different,” says Cindy Robin, a registered nurse at the Providence hospital, who has been caring for mothers and newborns for more than 30 years. “It’s a more distressed cry,” she says, “and it really pulls at your heartstrings to have to listen to them.”
Cindy Robin, a registered nurse at Women and Infants Hospital in Providence, R.I., helps newborns through symptoms of withdrawal. (Photo by Kristin Espeland Gourlay/RIPR)
Robin says babies with mild symptoms of the withdrawal syndrome will sneeze and sniffle. They have trouble settling down. Babies who have a more severe case can have seizures and dangerously high fevers. Robin says nurses have to dim the lights, and swaddle the newborns tightly to help keep them calm.
“They just need to be held in a nice, quiet spot,” she says. “We have nice quiet music playing, and try to keep them as comfortable as possible.”
Nurses with special training check on the babies every couple of hours.
“So these are the things that we look for … and what we teach the parents,” she says: “Is the baby crying excessively? Is it a high pitched cry? Is it just a continuous cry? How do they sleep after they eat?”
Medication, which is gradually decreased, can help ease this constellation of symptoms.
“The American Academy of Pediatrics and others recommend an opioid for the babies, because you’re giving them back what they’re withdrawing from,” explains Dr. Jonathan Davis, a neonatologist and chief of newborn medicine at Tufts’ Medical Center. “Morphine and methadone are the two most common.”
But Davis says no one’s really done the research to figure out which drug works better for babies, and doctors are left to figure that out by trial and error, case by case. Though the Food and Drug Administration hasn’t officially approved morphine or methadone for use in newborns, doctors prescribe these drugs to the children anyway, in smaller doses than they give adults.
“As I spoke to people around the country, everyone would have their own approach and a very different way of treating these babies,” Davis says. “And we thought that quite odd.”
So he and a colleague, Brown University developmental psychologist Barry Lester, have launched a major study to sort out what works best. The two are hoping to enroll 180 babies in their double-blind, randomized, controlled trial — no one will know which newborns are getting methadone, and which are getting morphine, for example, until the study’s end. And they’re taking the research further: No study yet has looked at the long-term effects of the drugs, so Davis and Lester will continue to follow-up with measures of cognitive and physical development until the children are 18 months old.
“It may be,” Davis says, “that one agent is safer short-term, but when we look longer-term it may actually be more dangerous.” Teasing out long-term effects of a drug isn’t easy, Lester says; many factors can influence a baby’s development.
“If you’re drug-exposed and you’re growing up in an inadequate environment — which may not be poverty, it may be inadequate parenting — that’s a double whammy,” he says. “Those are going to be your worst case scenarios.”
Despite many remaining unknowns, doctors have consistently found that treatment with morphine or methadone enables most babies to get through withdrawal in about six to eight weeks.
“It can be heartbreaking,” says Robin, who has helped shepherd many kids through dark days. “But at the end, it is also rewarding,” she says, “because you see them get better and you see them go home.”





9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))

 The Juneau Police Department is hosting an event Saturday to help heroin users and those who have lost someone to the drug. Hope, Not Heroin will have food, music and 31 booths with information about addiction and recovery.
The Juneau Police Department is hosting an event Saturday to help heroin users and those who have lost someone to the drug. Hope, Not Heroin will have food, music and 31 booths with information about addiction and recovery. 

9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))