Police form a line near Emancipation Park in Charlottesville, Virginia, amid Unite the Right protesters and counterprotesters on Aug. 12, 2017. (Creative Commons photo by Stephen Melkisethian)
Even before the demonstration in Virginia began last weekend, the police there knew they weren’t going to be able to handle what was coming.
Charlottesville police officers, including Sgt. Jake Via of the investigations bureau, had been contacting organizers and scanning social media to figure out how many demonstrators were headed their way and whether they would be armed.
“The number each group was saying was just building and building,” Via said. “We saw it coming. … Looking at this, I said, ‘This is going to be bad.’”
The protesters’ numbers were too large and the downtown park too small. City officials tried to get the demonstration moved to another, more spacious location, but lost in court after the rally’s organizer, backed by the American Civil Liberties Union, alleged his freedom of speech was being infringed.
The protests, of course, ended tragically. Local law enforcement was widely blamed for losing control of the event and standing back even as people were attacked.
Via maintains that nothing the police did could have stopped the violence between the two sides. “No hours and hours and hours or even months of planning is going to stop the radicals from both sides wanting to go at it,” he said.
With more demonstrations planned in cities across the country, ProPublica interviewed law enforcement experts in the United States and Europe to ask what more can be done to prevent bloodshed at protests where people are spoiling for a fight. The consensus was that additional steps can be taken.
But many of the tactics come at a price. Some could be viewed as impinging on civil liberties and the constitutionally enshrined rights to free assembly and protest. Others require funding and coordination that is difficult to achieve within the fragmented framework of American policing. A few are as simple as strategically placed blockades that keep the two sides separate. Here are some of the top approaches and how they might — or might not — be deployed in the U.S.
Drones, Anti-Mask Laws and Open-Carry Restrictions
Local police forces will increasingly institutionalize the use of drones at mass demonstrations. That’s the prediction of Brian Levin, a criminal justice professor at California State University, San Bernardino. Cameras in the air with real-time feeds transmitted to officers on the ground would allow police to cover more terrain and in some cases, identify potential conflicts before they erupt.
“Demonstrations spread, and these violent confrontations can take place in disparate areas,” said Levin. “It’s like when a hammer hits mercury.”
Drones can also be safer than helicopters. In Charlottesville, a helicopter monitoring the demonstration went down, killing two state troopers aboard.
But police drone use has been met with opposition from civil liberties groups. Drones donated to the Los Angeles Police Department have gone unused for years amid privacy concerns. Activists have argued that access to the devices, which make surveillance cheaper and more efficient, will lead police to more routinely surveil private citizens.
Earlier this month, LA’s police commission gathered to discuss relaunching the program only to be met by chanting activists who shut down the conversation twice. Similar stories have played out in Seattle and elsewhere.
Another tool cities and states (including Virginia) have used is anti-mask laws, which bar groups of people from disguising themselves in public. Violent demonstrators will sometimes arrive in ski masks or scarves wrapped around their faces. New York City has a ban, with exceptions including for Halloween. So does Alabama, a rule it instituted in 1949 to unmask the Ku Klux Klan. A similar restriction in California, though, was struck down after Iranian Americans hoping to safely (and non-violently) protest the post-revolutionary regime back home sued on First Amendment grounds.
Another challenge in Charlottesville was the number of demonstrators who came with guns, and were allowed to do so lawfully, because of Virginia’s open-carry laws.
Even in states with such statutes, the authorities have some options. Erwin Chemerinsky, dean of the University of California, Berkeley’s law school, said the Supreme Court has upheld the right to have guns at home, but not necessarily in public. “Think of curfews. The government has the ability to take steps to protect public safety,” Chemerinsky said. “The more evidence there is that it’s a threat to public safety, the more sympathetic the courts would be.”
The evidence could consist of past rallies that broke out into violence, or intelligence that an armed group is planning to employ force in the future.
Still, attempts to temporarily restrict gun rights have floundered in the past. Before the most recent Republican National Convention in Cleveland, the head of Cleveland’s largest police union and others called for the state’s open-carry laws to be tightened during the convention. Gov. John Kasich refused, saying “Ohio governors do not have the power to arbitrarily suspend federal and state constitutional rights.”
A more radical approach comes from Philip Zelikow, a history professor at the University of Virginia and former executive director of the 9/11 Commission. In 1981, he worked with the Southern Poverty Law Center, a civil rights nonprofit, to ask a federal judge to shut down a group called the Knights of the Ku Klux Klan, which was showing up armed and in Army-style clothing on the Texas Gulf Coast to harass Vietnamese fishermen.
With the support of the Texas attorney general, Zelikow and his team invoked a 19th-century law that forbids “military companies” not authorized by the governor. They argued that the Klan qualified because it was not government-regulated but had “command structure, training and discipline so as to function as a combat or combat support unit.” The lawyers prevailed, and the Klan was forced to leave its weapons at home.
A similar argument also succeeded soon after in North Carolina, and Zelikow said groups like those in Charlottesville that are mixing weaponry and political activism could be subject to similar legal challenges. “These problems haven’t come up much in recent decades,” Zelikow said. “The issue subsided and memory fades but here we are again.”
Most states have restrictions on private military-like groups. Zelikow was contacted by lawyers from Oklahoma this week, asking if their state had such a law on the books. “It took me about five minutes to find,” he said. Zelikow is now trying to form a team of lawyers to bring a case in Virginia.
Looking Abroad
Thousands of people, divided into two opposing sides, squaring off in public. Some come armed, looking to damage property and wreak havoc. Many filter in from out of town, complicating efforts by police to negotiate peace in advance.
It’s a scenario European authorities know well, though with a different kind of group: soccer hooligans.
Maria Haberfeld, a professor at the John Jay College of Criminal Justice in New York and a former supervisor in the Israel National Police, said cops in the Netherlands use a “situation-oriented” model to keep violent rival soccer fans under control.
That framework trains officers in perceptual skills, helping them develop the emotional intelligence to read members of crowds and make sound judgments about which situations are truly dangerous. Officers are put through simulations in which they can achieve positive, nonfatal outcomes. Trainings are handled in groups, not individually, so that in the field, officers are less likely to misinterpret any of their colleagues’ motions or actions.
“European police forces are light years ahead of us in terms of training.” Haberfeld said. “It’s not something you can train police officers to do in half an hour. It’s a serious commitment.”
Reaching that level of training may not be feasible in the U.S., where local municipalities set their own academy protocols. (And demonstrations are less frequent than soccer matches.) The training in the U.S. typically lasts just a few months, compared to the couple of years that European police cadets get.
In Germany, police forces commonly have specialized units assigned to each side of a potentially violent protest. Officers meet with the groups’ leaders in advance and discuss plans for the protest in detail, including symbols that are forbidden for display by the government.
Protest leaders can be denied permits to demonstrate because of criminal records, forcing them to turn leadership of the event over to another member of the group. They’re also asked to assign deputies from within their organization who can help the group’s leader keep things under control. Those assistants also have their records vetted by the police before being approved.
Once at the event, the specialized police units show up in distinctive yellow vests, and without riot gear, so they can mix in with the demonstrators less threateningly. When officers see someone with a banned weapon, they sometimes will only film the demonstrator and make an arrest later.
“It is important for us, is not to have a negative solidarity spillover effect. … If we disarm a person or act against a small group of potentially violent protestors, other people around solidarize with them against the police,” said Elke Heilig, head of the anti-conflict team in Pforzheim, Germany. “This leads towards escalation.”
Keeping Peaceful Protesters Away
Social media gives hate groups a new megaphone for getting the word out about their rallies, opening up communication with many previously fragmented niche groups and helping lead to larger gatherings, experts said. A big crowd is inherently harder to police, but what makes the scenario even more vexing for law enforcement is that they’re now dealing with not just one or two groups, but many, along with unaffiliated individuals.
“People are coming in from disparate places and disparate groups who don’t answer to any single authority. A Klan leader can tell his folks to stand down,” said Levin, a former NYPD officer. “Social media has been a magnet not only for haters but for unstable haters.”
Some municipalities are responding by using social media tools to dissuade some activists from showing up. City officials in Berkeley, California, have experimented with discouraging peaceful protesters from attending demonstrations they expect to be violent.
In March, fights broke out between supporters and opponents of the president at a demonstration near the Berkeley campus. Some of the unruly counter-protesters were believed to be affiliated with black bloc, an anarchist group whose members are known to wear black and mask their faces. Mayhem ensued. In one case, a man wearing a “Trump is My President” shirt had his face bloodied.
“There are people who come intent on committing violence and they look for ways to subvert whatever you set up,” said city spokesman Matthai Chakko. “There are people who use peaceful protesters as shields. They blend into crowds after they commit their acts.”
In April, before another planned demonstration, the city launched a messaging campaign suggesting peaceful protesters keep their distance. “Consider whether the approach others advertise is the style and venue for you,” one alert read, warning of violent protesters. “Reaching out to organizations or individuals in need is an alternative to conflict. When people at an event act in a way that compromises your values and goals, separate yourself.”
The number of peaceful protesters dropped significantly, Chakko said, and the city is taking a similar approach with an unpermitted, white nationalist demonstration expected later this month. The alert the city sent out Wednesday was direct: “The best response for those seeking to safeguard our community is to stay away.”
Barriers and Chain-Link Fences
Miriam Krinsky, a former federal prosecutor who has worked on police reform efforts in Los Angeles, said the most fundamental strategy for dueling demonstrations is keeping the two sides separate, with physical obstacles and police in between. “Create a human barrier so the flash points are reduced as quickly as possible,” she said.
Law enforcement will sometimes quarantine protesting hate groups inside concentric chain link fences, creating a large empty space between opposing groups. Those entering the inner ring are sent through metal detectors.
At an anti-Sharia protest in San Bernardino, California earlier this year, the two groups were kept on opposite sides of the street, with horse-mounted cops there to prevent protesters from crossing over.
The lack of space to separate the factions was a widely noted problem in Charlottesville. The massive demonstration was allowed to take place inside a small downtown park, making it more difficult for police to insert themselves and separate the two sides. “The two groups are both trying to occupy the same area and this doesn’t give police a lot of maneuverability,” said John Kleinig, professor emeritus at John Jay College of Criminal Justice.
Demonstrators ended up spilling out beyond the park, and one counter-protester was killed when an Ohio man allegedly plowed his car into a crowd a few blocks away from the park.
Demonstrations can in some ways be easier to control in concentrated urban areas, where police use tall buildings with little or no space in between them as barriers. And smaller city police forces generally have less training in large crowd control.
“I’m former NYPD,” Levin said. “We had grid patterns and streets we could block off, put a wedge in when we had an unruly crowds. … You have people hemmed in by structures and street grid patterns. In smaller places, people can spread out in all different directions.”
Since the weekend, amid criticism of their handling of the demonstration, Charlottesville Police Chief Al Thomas acknowledged that crowd’s spread led to problems.
“We had to actually send out forces to multiple locations to deal with a number of disturbances,” he said. “It was certainly a challenge. We were spread thin once the groups dispersed.”
Special correspondent Pia Dangelmayer in Germany contributed to this story.
Sam Clovis speaks at a campaign rally for Republican presidential candidate Donald Trump at Iowa State University in Ames, Iowa, on Jan. 19, 2016. President Trump is likely to appoint him to a an undersecretary position in the USDA that serves as the agency’s chief scientist — though he’s not a scientist. (Creative Commons photo by Alex Hanson)
The USDA’s research section studies everything from climate change to nutrition. Under the 2008 Farm Bill, its leader is supposed to serve as the agency’s “chief scientist” and be chosen “from among distinguished scientists with specialized or significant experience in agricultural research, education, and economics.”
But Sam Clovis — who, according to sources with knowledge of the appointment and members of the agriculture trade press, is President Trump’s pick to oversee the section — appears to have no such credentials.
Clovis has never taken a graduate course in science and is openly skeptical of climate change. While he has a doctorate in public administration and was a tenured professor of business and public policy at Morningside College for 10 years, he has published almost no academic work.
Clovis is better known for hosting a conservative talk radio show in his native Iowa and, after mounting an unsuccessful run for Senate in 2014, becoming a fiery pro-Trump advocate on television.
Clovis advised Trump on agricultural issues during his presidential campaign and is currently the senior White House adviser within the USDA, a position described by The Washington Post as “Trump’s eyes and ears” at the agency.
Clovis was also responsible for recruiting Carter Page, whose ties to Russia have become the subject of intense speculation and scrutiny, as a Trump foreign policy adviser.
Neither Clovis, nor the USDA, nor the White House responded to questions about Clovis’ nomination to be the USDA’s undersecretary for research, education and economics.
Catherine Woteki, who served as undersecretary for research, education and economics in the Obama administration, compared the move to appointing someone without a medical background to lead the National Institutes of Health. The USDA post includes overseeing scientific integrity within the agency.
“This position is the chief scientist of the Department of Agriculture. It should be a person who evaluates the scientific body of evidence and moves appropriately from there,” she said in an interview.
Woteki holds a Ph.D. in human nutrition and served as the first undersecretary for food safety at the USDA during the Clinton administration. She was then the dean of the school of agriculture at Iowa State University before becoming the global director of scientific affairs for Mars, Inc.
Clovis has a B.S. in political science from the U.S. Air Force Academy, an MBA from Golden State University and a doctorate in public administration from the University of Alabama. The University of Alabama canceled the program the year after Clovis graduated, but an old course catalogue provided by the university does not indicate the program required any science courses.
Clovis’ published works do not appear to include any scientific papers. His 2006 dissertation concerned federalism and homeland security preparation, and a search for academic research published by Clovis turned up a handful of journal articles, all related to national security and terrorism.
As undersecretary for research, education and economics, Woteki directed additional resources to helping local farmers and agricultural workers address the impacts of severe drought, flooding and unpredictable weather patterns. She chaired the “Global Research Alliance to Reduce Agricultural Greenhouse Gasses,” which brings together chief agricultural scientists from across the globe. Under her leadership, the USDA also created “Climate Hubs” across the country to help localized solutions for adapting to climate change.
Clovis has repeatedly expressed skepticism over climate science and has called efforts to address climate change “simply a mechanism for transferring wealth from one group of people to another.” He has indicated the Trump administration will take a starkly different approach at the USDA. Representing the campaign at the Farm Foundation Forum in October, Clovis told E&E News that Trump’s agriculture policy would focus on boosting trade and lessening regulation and not the impact of climate change.
“I think our position is very clearly [that] Mr. Trump is a skeptic on climate change, and we need more science,” he said. “Once we get more science, we are going to make decisions.”
The USDA’s undersecretary for research, education and economics has historically consulted on a wide range of scientific issues. Woteki, for example, said she was asked for input on the Zika and Ebola outbreaks because of the USDA’s relevant research and was frequently called upon to offer guidance on homeland security issues related to food safety.
“Access to safe food and clean air and water is absolutely fundamental to personal security,” she said, adding that a scientific understanding of food safety is critical to success in the job. “Food systems are widely recognized by the national security community as being part of critical infrastructure.”
Clovis’ academic background includes years of study on homeland security, but focused almost exclusively on foreign policy. A biography he provided to the 2016 Fiscal Summit at which he was a speaker indicates he is “a federalism scholar” and “an expert on homeland security issues,” with “regional expertise in Europe, the former Soviet Union, and the Middle East.” Neither this biography nor any other publicly available biographies list any experience in food safety, agriculture or nutrition.
Clovis first became well-known in Iowa through his radio show, “Impact with Sam Clovis.” He finished a distant second in the 2014 Republican Primary for an Iowa Senate seat ultimately won by Joni Ernst. During the race, his outlandish statements often made headlines. In one instance, he said the only reason President Obama hadn’t yet been impeached was because of his race.
While he initially signed on as former Texas Gov. Rick Perry’s top Iowa adviser, he left in August 2015 to become the Trump campaign’s national co-chair and chief policy adviser. Emails leaked by the Perry campaign to The Des Moines Register show Clovis slamming Trump in the months before, questioning his faith. “His comments reveal no foundation in Christ, which is a big deal,” Clovis wrote. He also praised Perry for calling Trump a “cancer on conservatism.”
Still, Clovis subsequently became one of Trump’s best-known advocates on cable television, where he relentlessly defended his new boss. On “Morning Joe,” he said Democratic presidential nominee Hillary Clinton had failed to “control the sexual predation that went on in her own home.” On SiriusXM, he said Republicans who were abandoning Trump were “weak-kneed” and “lily-livered.”
Trump’s call for a “total and complete shutdown” of entry of Muslims into the United States in December 2015 put Clovis’ job as a tenured professor at risk.
“If he played a role in drafting or advising the Trump campaign on this issue, we will be outraged and extremely disappointed in Dr. Clovis,” Morningside College spokesman Rick Wollman told Iowa Starting Line, before pledging to look “more closely” at the issue.
Clovis went on unpaid leave from the college in the summer of 2015 and resigned after Trump’s win in November.
Do you have information about this case or other Trump administration appointees? Contact Jessica Huseman at jessica.huseman@propublica.org or via Signal at 972-268-1882.
Photographs of Lauren and Larry in the Bloomstein’s home in New Jersey. Bryan Anselm for ProPublica
As a neonatal intensive care nurse, Lauren Bloomstein had been taking care of other people’s babies for years. Finally, at 33, she was expecting one of her own. The prospect of becoming a mother made her giddy, her husband Larry recalled recently— “the happiest and most alive I’d ever seen her.”
When Lauren was 13, her own mother had died of a massive heart attack. Lauren had lived with her older brother for a while, then with a neighbor in Hazlet, N.J., who was like a surrogate mom, but in important ways, she’d grown up mostly alone. The chance to create her own family, to be the mother she didn’t have, touched a place deep inside her.
“All she wanted to do was be loved,” said Frankie Hedges, who took Lauren in as a teenager and thought of her as her daughter. “I think everybody loved her, but nobody loved her the way she wanted to be loved.”
Other than some nausea in her first trimester, the pregnancy went smoothly. Lauren was “tired in the beginning, achy in the end,” said Jackie Ennis, her best friend since high school, who talked to her at least once a day. “She gained what she’s supposed to. She looked great, she felt good, she worked as much as she could” — at least three 12-hour shifts a week until late into her ninth month. Larry, a doctor, helped monitor her blood pressure at home, and all was normal.
On her days off she got organized, picking out strollers and car seats, stocking up on diapers and onesies. After one last pre-baby vacation to the Caribbean, she and Larry went hunting for their forever home, settling on a brick colonial with black shutters and a big yard in Moorestown, N.J., not far from his new job as an orthopedic trauma surgeon in Camden. Lauren wanted the baby’s gender to be a surprise, so when she set up the nursery she left the walls unpainted — she figured she’d have plenty of time to choose colors later. Despite all she knew about what could go wrong, she seemed untroubled by the normal expectant-mom anxieties. Her only real worry was going into labor prematurely. “You have to stay in there at least until 32 weeks,” she would tell her belly. “I see how the babies do before 32. Just don’t come out too soon.”
When she reached 39 weeks and six days — Friday, Sept. 30, 2011 — Larry and Lauren drove to Monmouth Medical Center in Long Branch, the hospital where the two of them had met in 2004 and where she’d spent virtually her entire career. If anyone would watch out for her and her baby, Lauren figured, it would be the doctors and nurses she worked with on a daily basis. She was especially fond of her obstetrician/gynecologist, who had trained as a resident at Monmouth at the same time as Larry. Lauren wasn’t having contractions, but she and the ob/gyn agreed to schedule an induction of labor — he was on call that weekend and would be sure to handle the delivery himself.
Inductions often go slowly, and Lauren’s labor stretched well into the next day. Ennis talked to her on the phone several times: “She said she was feeling okay, she was just really uncomfortable.” At one point, Lauren was overcome by a sudden, sharp pain in her back near her kidneys or liver, but the nurses bumped up her epidural and the stabbing stopped.
Inductions have been associated with higher cesarean-section rates, but Lauren progressed well enough to deliver vaginally. On Saturday, Oct. 1, at 6:49 p.m., 23 hours after she checked into the hospital, Hailey Anne Bloomstein was born, weighing 5 pounds, 12 ounces. Larry and Lauren’s family had been camped out in the waiting room; now they swarmed into the delivery area to ooh and aah, marveling at how Lauren seemed to glow.
Larry floated around on his own cloud of euphoria, phone camera in hand. In one 35-second video, Lauren holds their daughter on her chest, stroking her cheek with a practiced touch. Hailey is bundled in hospital-issued pastels and flannel, unusually alert for a newborn; she studies her mother’s face as if trying to make sense of a mystery that will never be solved. The delivery room staff bustles in the background in the low-key way of people who believe everything has gone exactly as it’s supposed to.
Then Lauren looks directly at the camera, her eyes brimming.
Twenty hours later, she was dead.
“We don’t pay enough attention”
The ability to protect the health of mothers and babies in childbirth is a basic measure of a society’s development. Yet every year in the U.S., 700 to 900 women die from pregnancy or childbirth-related causes, and some 65,000 nearly die — by many measures, the worst record in the developed world.
American women are more than three times as likely as Canadian women to die in the maternal period (defined by the Centers for Disease Control as the start of pregnancy to one year after delivery or termination), six times as likely to die as Scandinavians. In every other wealthy country, and many less affluent ones, maternal mortality rates have been falling; in Great Britain, the journal Lancet recently noted, the rate has declined so dramatically that “a man is more likely to die while his partner is pregnant than she is.” But in the U.S., maternal deaths increased from 2000 to 2014. In a recent analysis by the CDC Foundation, nearly 60 percent of such deaths are preventable.
While maternal mortality is significantly more common among African-Americans, low-income women and in rural areas, pregnancy and childbirth complications kill women of every race and ethnicity, education and income level, in every part of the U.S. ProPublica and NPR spent the last several months scouring social media and other sources, ultimately identifying more than 450 expectant and new mothers who have died since 2011.
The list includes teachers, insurance brokers, homeless women, journalists, a spokeswoman for Yellowstone National Park, a co-founder of the YouTube channel WhatsUpMoms, and more than a dozen doctors and nurses like Lauren Bloomstein. They died from cardiomyopathy and other heart problems, massive hemorrhage, blood clots, infections and pregnancy-induced hypertension (preeclampsia) as well as rarer causes. Many died days or weeks after leaving the hospital. Maternal mortality is commonplace enough that three new mothers who died, including Lauren, were cared for by the same ob/gyn.
The reasons for higher maternal mortality in the U.S. are manifold. New mothers are older than they used to be, with more complex medical histories. Half of pregnancies in the U.S. are unplanned, so many women don’t address chronic health issues beforehand. Greater prevalence of C-sections leads to more life-threatening complications. The fragmented health system makes it harder for new mothers, especially those without good insurance, to get the care they need. Confusion about how to recognize worrisome symptoms and treat obstetric emergencies makes caregivers more prone to error.
Yet the worsening U.S. maternal mortality numbers contrast sharply with the impressive progress in saving babies’ lives. Infant mortality has fallen to its lowest point in history, the CDC reports, reflecting 50 years of efforts by the public health community to prevent birth defects, reduce preterm birth, and improve outcomes for very premature infants. The number of babies who die annually in the U.S. — about 23,000 in 2014 — still greatly exceeds the number of expectant and new mothers who die, but the ratio is narrowing.
The divergent trends for mothers and babies highlight a theme that has emerged repeatedly in ProPublica‘s and NPR’s reporting. In recent decades, under the assumption that it had conquered maternal mortality, the American medical system has focused more on fetal and infant safety and survival than on the mother’s health and wellbeing.
At the federally funded Maternal-Fetal Medicine Units Network, the preeminent obstetric research collaborative in the U.S., only four of the 34 initiatives listed in its online database primarily target mothers, versus 24 aimed at improving outcomes for infants (the remainder address both).
Under the Title V federal-state program supporting maternal and child health, states devoted about 6 percent of block grants in 2016 to programs for mothers, compared to 78 percent for infants and special-needs children. The notion that babies deserve more care than mothers is similarly enshrined in the Medicaid program, which pays for about 45 percent of births. In many states, the program covers moms for 60 days postpartum, their infants for a full year. The bill to replace the Affordable Care Act, adopted by the U.S. House of Representatives earlier this month, could gut Medicaid for mothers and babies alike.
At the provider level, advances in technology have widened the gap between maternal and fetal and infant care. “People became really enchanted with the ability to do ultrasound, and then high-resolution ultrasound, to do invasive procedures, to stick needles in the amniotic cavity,” said William Callaghan chief of the CDC’s Maternal and Infant Health Branch.
The growing specialty of maternal-fetal medicine drifted so far toward care of the fetus that as recently as 2012, young doctors who wanted to work in the field didn’t have to spend time learning to care for birthing mothers. “The training was quite variable across the U.S.,” said Mary D’Alton, chair of ob/gyn at Columbia University Medical Center and author of papers on disparities in care for mothers and infants. “There were some fellows that could finish their maternal-fetal medicine training without ever being in a labor and delivery unit.”
In the last decade or so, at least 20 hospitals have established multidisciplinary fetal care centers for babies at high risk for a variety of problems. So far, only one hospital in the U.S. — NewYork-Presbyterian/Columbia —has a similar program for high-risk moms-to-be.
In regular maternity wards, too, babies are monitored more closely than mothers during and after birth, maternal health advocates told ProPublica and NPR. Newborns in the slightest danger are whisked off to neonatal intensive care units like the one Lauren Bloomstein worked at, staffed by highly trained specialists ready for the worst, while their mothers are tended by nurses and doctors who expect things to be fine and are often unprepared when they aren’t.
When women are discharged, they routinely receive information about how to breastfeed and what to do if their newborn is sick but not necessarily how to tell if they need medical attention themselves. “It was only when I had my own child that I realized, ‘Oh my goodness. That was completely insufficient information,'” said Elizabeth Howell, professor of obstetrics and gynecology at the Icahn School of Medicine at Mount Sinai Hospital in New York City.
“The way that we’ve been trained, we do not give women enough information for them to manage their health postpartum. The focus had always been on babies and not on mothers.”
In 2009, the Joint Commission, which accredits 21,000 health care facilities in the U.S., adopted a series of perinatal “core measures” — national standards that have been shown to reduce complications and improve patient outcomes. Four of the measures are aimed at making sure the baby is healthy. One — bringing down the C-section rate— addresses maternal health.
Meanwhile, life-saving practices that have become widely accepted in other affluent countries — and in a few states, notably California — have yet to take hold in many American hospitals. Take the example of preeclampsia, a type of high blood pressure that only occurs in pregnancy or the postpartum period, and can lead to seizures and strokes. Around the world, it kills an estimated five women an hour. But in developed countries, it is highly treatable. The key is to act quickly.
By standardizing its approach, Britain has reduced preeclampsia deaths to one in a million — a total of two deaths from 2012 to 2014. In the U.S., on the other hand, preeclampsia still accounts for about 8 percent of maternal deaths— 50 to 70 women a year. Including Lauren Bloomstein.
“I cannot remember too many health care employees that I respect as much as Lauren”
When Lauren McCarthy Bloomstein was a teenager in the 1990s, a neighbor who worked for a New York publishing firm approached her about modeling for a series of books based on Louisa May Alcott’s classic “Little Women.” Since her mother’s death, Lauren had become solitary and shy; she loved to read, but she decided she wasn’t interested. “Are you kidding? Go do it!” Frankie Hedges insisted. “That would be fabulous!”
Lauren relented, and the publisher cast her as the eldest March sister, Meg. She appeared on the covers of four books, looking very much the proper 19th-century young lady with her long brown hair parted neatly down the middle and a string of pearls around her neck. The determined expression on her face, though, was pure Lauren.
“She didn’t want sympathy, she didn’t want pity,” Jackie Ennis said. “She wasn’t one to talk much about her feelings [about] her mom. She looked at it as this is what she was dealt and she’s gonna do everything in her power to become a productive person.”
In high school, Lauren decided her path lay in nursing, and she chose a two-year program at Brookdale Community College. She worked at a doctor’s office to earn money for tuition and lived in the garage apartment that Hedges and her husband had converted especially for her, often helping out with their young twin sons. Lauren “wasn’t a real mushy person,” Hedges said. “She wasn’t the type to say things like ‘I love you. ‘” But she clearly relished being part of a family again. “You can’t believe how happy she is,” Ennis once told Hedges. “We’ll be out and she’ll say, ‘Oh, I have to go home for dinner!'”
After graduating in 2002, Lauren landed at Monmouth Medical Center, a sprawling red-brick complex a few minutes from the ocean that is part of the RWJBarnabas Health system and a teaching affiliate of Philadelphia’s Drexel University College of Medicine. Her first job was in the medical surgical unit, where her clinical skills and work ethic soon won accolades.
“I cannot remember too many health care employees that I respect as much as Lauren,” Diane Stanaway, then Monmouth’s clinical director of nursing wrote in a 2005 commendation. “What a dynamite young lady and nurse!” When a top hospital executive needed surgery, Larry recalled, he paid Lauren the ultimate compliment, picking her as one of two private-duty nurses to help oversee his care.
Larry Bloomstein, who joined the unit as an orthopedic surgical resident in 2004, was dazzled, too. He liked her independent streak — “she didn’t feel the need to rely on anyone else for anything” — and her level-headedness. Even performing CPR on a dying patient, Lauren “had a calmness about her,” Larry said.
Larry and Lauren Bloomstein met at the hospital in 2004. They married five years later. Courtesy of the Bloomstein Family
He thought her tough upbringing “gave her a sense of confidence. She didn’t seem to worry about small things.” Lauren, meanwhile, told Ennis, “I met this guy. He’s a doctor, and he’s very kind.” Their first date was a Bruce Springsteen concert; five years later they married on Long Beach Island, on the Jersey shore.
One of Lauren’s favorite books was “Catcher in the Rye” — “she related to the Holden Caulfield character rescuing kids,” Larry said. When a spot opened at Monmouth’s elite neonatal intensive care unit in 2006, she jumped at it.
The hospital has the fifth-busiest maternity department in the state, delivering 5,449 babies in 2016. Monmouth earned an “A” grade from Leapfrog, a nonprofit that promotes safety in health care, and met full safety standards in critical areas of maternity care, such as rates of C-sections and early elective deliveries, a hospital spokeswoman said. Its NICU, a Level III facility for high-risk newborns, is the oldest in New Jersey.
“With NICU nursing, it’s one of those things either you get it or you don’t,” said Katy DiBernardo, a 20-year veteran of the unit. “The babies are little, and a lot of people aren’t used to seeing a teeny tiny baby.” The NICU staff included nurses, neonatologists, a respiratory therapist, and residents. Lauren, DiBernardo said, “just clicked.”
One of the things Lauren liked best about her work was the bonds she formed with babies’ families. Nurses followed the same newborns throughout their stay, sometimes for weeks or months. She was a touchstone for parents — very good at “calming people down who have a lot of anxiety,” Larry said — and often stayed in contact long after the babies went home, meeting the moms for coffee and even babysitting on occasion.
She also cherished the deep friendships that a place like the NICU forged. The neonatal floor was like a world unto itself, Lauren Byron, another long-time nurse there, explained: “There’s a lot of stress and pressure, and you are in life-and-death situations. You develop a very close relationship with some people.”
The environment tended to attract very strong personalities. Lauren’s nickname in the Bloomstein family football pool was “The Feisty One,” so she fit right in. But she could stand her ground without alienating anyone. “She was one of those people that everyone liked,” Byron said.
Monmouth Medical Center in Long Branch, N.J., the hospital where Lauren and Larry had met in 2004. Bryan Anselm for ProPublica
“We save more than we lose”
Another person everyone liked was ob/gyn John Vaclavik. He had come to Monmouth as a resident in 2004, around the same time as Larry, after earning his bachelor’s from Loyola College in Baltimore and his medical degree at St. George’s University on the island of Grenada. Medicine was the family profession: two uncles and two brothers also became doctors and his wife was a perinatal social worker at the hospital. Lauren and her colleagues thought he was “very personable” and “a great guy,” Larry said.
“She was good friends with my wife and she felt comfortable with me,” Vaclavik would recall in a 2015 court deposition.
After his residency, Vaclavik joined Ocean Obstetric & Gynecologic Associates, a thriving practice that counted numerous medical professionals among its clients. Vaclavik was a “laborist” — part of a movement that aimed to reduce the number of C-sections, which tend to have more difficult recoveries and more complications than vaginal births. In a state with a C-section rate of 37 percent, Monmouth’s rate in 2016 was just 21 percent.
The neonatal nurses had plenty of opportunity to observe Vaclavik and other ob/gyns in action—someone from NICU was called to attend every delivery that showed signs of being complicated or unusual as well as every C-section. “We always laughed, ‘They’ll call us for a hangnail,'” DiBernardo said. Lauren was so impressed by Vaclavik that she not only chose him as her own doctor, she recommended him to her best friend. “She kept saying, ‘You have to go to this guy. He’s a good doctor. Good doctor,'” Ennis said.
In other ways, though, the NICU staff and the labor and delivery staff were very separate. The neonatal nurses were focused on their own fragile patients — the satisfaction that came from helping them grow strong enough to go home, the grief when that didn’t happen. Once Ennis asked Lauren, “How do you deal with babies that don’t make it? That’s got to be so bad.” Lauren replied, “Yeah, but we save more than we lose.”
Loss was less common in labor and delivery, and when a new mother suffered life-threatening complications, the news did not always reach the NICU floor. Thus, when a 29-year-old special education teacher named Tara Hansen contracted a grisly infection a few days after giving birth to her first child in March 2011, the tragedy didn’t register with Lauren, who was then three months’ pregnant herself.
Hansen lived in nearby Freehold, N.J., with her husband, Ryan, her high school sweetheart. Her pregnancy, like Lauren’s, had been textbook perfect and she delivered a healthy nine-pound son. But Hansen suffered tearing near her vagina during childbirth. She developed signs of infection but was discharged anyway, a lawsuit by her husband later alleged.
Hansen was soon readmitted to Monmouth with what the lawsuit called “excruciating, severe pain beyond the capacity of a human being to endure.” The diagnosis was necrotizing fasciitis, commonly known as flesh-eating bacteria; two days later Hansen was dead. One of Vaclavik’s colleagues delivered Hansen’s baby; Vaclavik himself authorized her discharge. According to court documents, he said nurses failed to inform him about Hansen’s symptoms and that if he’d known her vital signs weren’t stable, he wouldn’t have released her. The hospital and nurses eventually settled for $1.5 million. The suit against Vaclavik and his colleagues is pending.
Vaclavik did not respond to several interview requests from ProPublica and NPR, including an emailed list of questions. “Due to the fact this matter is in litigation,” his attorney responded, “Dr. Vaclavik respectfully declines to comment.”
Citing patient privacy, Monmouth spokeswoman Elizabeth Brennan also declined to discuss specific cases. “We are saddened by the grief these families have experienced from their loss,” she said in a statement.
“I don’t feel good”
Larry Bloomstein’s first inkling that something was seriously wrong with Lauren came about 90 minutes after she gave birth. He had accompanied Hailey up to the nursery to be weighed and measured and given the usual barrage of tests for newborns. Lauren hadn’t eaten since breakfast, but he returned to find her dinner tray untouched. “I don’t feel good,” she told him. She pointed to a spot above her abdomen and just below her sternum, close to where she’d felt the stabbing sensation during labor. “I’ve got pain that’s coming back.”
Larry had been at Lauren’s side much of the previous 24 hours. Conscious that his role was husband rather than doctor, he had tried not to overstep. Now, though, he pressed Vaclavik: What was the matter with his wife? “He was like, ‘I see this a lot. We do a lot of belly surgery. This is definitely reflux,'” Larry recalled. According to Lauren’s records, the ob/gyn ordered an antacid called Bicitra and an opioid painkiller called Dilaudid. Lauren vomited them up.
Lauren’s pain was soon 10 on a scale of 10, she told Larry and the nurses; so excruciating, the nurses noted, “Patient [is] unable to stay still.” Just as ominously, her blood pressure was spiking. An hour after Hailey’s birth, the reading was 160/95; an hour after that, 169/108. At her final prenatal appointment, her reading had been just 118/69. Obstetrics wasn’t Larry’s specialty, but he knew enough to ask the nurse: Could this be preeclampsia?
Preeclampsia, or pregnancy-related hypertension, is a little-understood condition that affects 3 percent to 5 percent of expectant or new mothers in the U.S., up to 200,000 women a year. It can strike anyone out of the blue, though the risk is higher for African Americans, women with preexisting conditions such as obesity, diabetes or kidney disease, and mothers over the age of 40. It is most common during the second half of pregnancy, but can develop in the days or weeks after childbirth, and can become very dangerous very quickly. Because a traditional treatment for preeclampsia is to deliver as soon as possible, the babies are often premature and end up in NICUs like the one where Lauren worked.
As Larry suspected, Lauren’s blood pressure readings were well past the danger point. What he didn’t know was that they’d been abnormally high since she entered the hospital — 147/99, according to her admissions paperwork. During labor, she had 21 systolic readings at or above 140 and 13 diastolic readings at or above 90, her records indicated; for a stretch of almost eight hours, her blood pressure wasn’t monitored at all, the New Jersey Department of Health later found. Over that same period, her baby’s vital signs were being constantly watched, Larry said.
In his court deposition, Vaclavik described the 147/99 reading as “elevated” compared to her usual readings, but not abnormal. He “would use 180 over 110 as a cutoff” to suspect preeclampsia, he said. Still, he acknowledged, Lauren’s blood pressure “might have been recommended to be monitored more closely, in retrospect.”
Leading medical organizations in the U.S. and the U.K. take a different view. They advise that increases to 140/90 for pregnant women with no previous history of high blood pressure signify preeclampsia. When systolic readings hit 160, treatment with anti-hypertensive drugs and magnesium sulfate to prevent seizures “should be initiated ASAP,” according to guidelines from the Alliance for Innovation on Maternal Health.
When other symptoms, such as upper abdominal (epigastric) pain, are present, the situation is considered even more urgent.
This basic approach isn’t new: “Core Curriculum for Maternal-Newborn Nursing,” a widely-used textbook, outlined it in 1997. Yet failure to diagnose preeclampsia, or to differentiate it from chronic high blood pressure, is all too common.
California researchers who studied preeclampsia deaths over several years found one striking theme: “Despite triggers that clearly indicated a serious deterioration in the patient’s condition, health care providers failed to recognize and respond to these signs in a timely manner, leading to delays in diagnosis and treatment.”
Preeclampsia symptoms — swelling and rapid weight gain, gastric discomfort and vomiting, headache and anxiety — are often mistaken for the normal irritations that crop up during pregnancy or after giving birth. “We don’t have a yes-no test for it,” said Eleni Tsigas, executive director of the Preeclampsia Foundation. “A lot of physicians don’t necessarily see a lot of it.”
Outdated notions – for example, that delivering the baby cures the condition – unfamiliarity with best practices and lack of crisis preparation can further hinder the response.
The fact that Lauren gave birth over the weekend may also have worked against her. Hospitals may be staffed differently on weekends, adding to the challenges of managing a crisis. A new Baylor College of Medicine analysis of 45 million pregnancies in the U.S. from 2004 to 2014 found mothers who deliver on Saturday or Sunday have nearly 50 percent higher mortality rates as well as more blood transfusions and more perineal tearing. The “weekend effect” has also been associated with higher fatality rates from heart attacks, strokes and head trauma.
According to Lauren’s records, Vaclavik did order a preeclampsia lab test around 8:40 p.m., but a nurse noted a half-hour later: “No abnormal labs present.” (According to Larry, the results were borderline.) Larry began pushing to call in a specialist. Vaclavik attributed Lauren’s pain to esophagitis, or inflammation of the esophagus, which had afflicted her before, he said in his deposition. Around 10 p.m., according to Lauren’s medical records, he phoned the on-call gastroenterologist, who ordered an x-ray and additional tests, more Dilaudid and different antacids — Maalox and Protonix. Nothing helped.
Meanwhile, Larry decided to reach out to his own colleagues in the trauma unit at Cooper University Hospital in Camden. In his training, perhaps the most important lesson he’d learned was to ask for help: “If there’s a problem, I will immediately get another physician involved.” By chance, the doctor on call happened to be a fairly new mother. As Larry described Lauren’s symptoms, she interrupted him. “You can stop talking. I know what this is.” She said Lauren had HELLP syndrome, an acronym for the most severe variation of preeclampsia, characterized by hemolysis, or the breakdown of red blood cells; elevated liver enzymes; and low platelet count, a clotting deficiency that can lead to excessive bleeding and hemorrhagic stroke.
Larry’s colleague urged him to stop wasting time, he recalled. Lauren’s very high blood pressure, the vomiting, and the terrible pain radiating from her kidneys and liver were symptoms of rapid deterioration. “Your wife’s in a lot of danger,” the trauma doctor said. (She didn’t respond to ProPublica’s and NPR’s requests for comment.)
“It’s never just one thing”
Earlier this year, an analysis by the CDC Foundation of maternal mortality data from four states identified more than 20 “critical factors” that contributed to pregnancy-related deaths. Among the ones involving providers: lack of standardized policies, inadequate clinical skills, failure to consult specialists and poor coordination of care. The average maternal death had 3.7 critical factors.
“It’s never just one thing,” said Roberta Gold, a member of the Council on Patient Safety in Women’s Health Care, whose daughter and unborn grandson died from a pregnancy-related blood clot in 2010. “It’s always a cascading combination of things. It’s a slow-motion train wreck.”
The last 16 hours of Lauren’s life were consistent with that grim pattern. Distressed by what the trauma doctor had told him, Larry immediately went to Lauren’s caregivers. But they insisted the tests didn’t show preeclampsia, he said. Not long after, Larry’s colleague called back to check on Lauren’s condition. “I don’t believe those labs,” he recalls her telling him. “They can’t be right. I’m positive of my diagnosis. Do them again.'”
Meanwhile, Lauren’s agony had become almost unendurable. The blood pressure cuff on her arm was adding to her discomfort, so around 10:30 p.m. her nurse decided to remove it — on the theory, Larry said, “We know her blood pressure is high. There’s no point to retaking it.” According to Lauren’s records, her blood pressure went unmonitored for another hour and 44 minutes.
Larry had given up on getting a specialist to come to the hospital so late on a Saturday night, but he persuaded Vaclavik to call in a general surgical resident. Around 11:55 p.m., according to the nurses’ notes, Lauren begged, “Do anything to stop this pain.” Vaclavik prescribed morphine, to little effect.
Just after midnight, her blood pressure about to peak at 197/117, Lauren began complaining of a headache. As Larry studied his wife’s face, he realized something had changed. “She suddenly looks really calm and comfortable, like she’s trying to go to sleep.” She gave Larry a little smile, but only the right side of her mouth moved.
In an instant, Larry’s alarm turned to panic. He ordered Lauren, “Lift your hands for me.” Only her right arm fluttered. He peeled off her blankets and scraped the soles of her feet with his fingernail, testing her so-called Babinski reflex; in an adult whose brain is working normally, the big toe automatically jerks downward. Lauren’s right toe curled as it was supposed to. But her left toe stuck straight out, unmoving. As Larry was examining her, Lauren suddenly seemed to realize what was happening to her. “She looked at me and said, ‘I’m afraid,’ and, ‘I love you.’ And I’m pretty sure in that moment she put the pieces together. That she had a conscious awareness of … that she was not going to make it.”
A CT scan soon confirmed the worst: The escalating blood pressure had triggered bleeding in her brain. So-called hemorrhagic strokes tend to be deadlier than those caused by blood clots. Surgery can sometimes save the patient’s life, but only if it is performed quickly.
Larry was a realist; he knew that even the best-case scenario was devastating. Chances were that Lauren would be paralyzed or partially paralyzed. She’d never be the mother she had dreamed of being. She’d never be a nurse again. But at least there was a chance she would live. When the neurologist arrived, Larry asked, “Is there hope here?” As he recalls it, the neurologist responded, “That’s why I’m here. There’s hope.”
Larry began gathering Lauren’s loved ones — his parents, her brother, Frankie Hedges and her husband Billy, Jackie Ennis. On the phone, he tried to play down the gravity of the situation, but everyone understood. When Larry’s mother arrived, the hospital entrance was locked, and Larry and Vaclavik came to meet her. “The obstetrician just said, ‘She’s going to be all right,'” Linda Bloomstein said. “And Larry was standing behind him, and I saw the tears coming down, and he was shaking his head, ‘No.'”
Around 2 a.m., the neurosurgeon finally confirmed what the trauma doctor had said four hours before: Lauren had HELLP syndrome. Then he delivered more bad news: Her blood platelets — essential to stopping the hemorrhage — were dangerously low. But, according to Larry, the hospital didn’t have sufficient platelets on site, so her surgery would have to be delayed. Larry was dumbfounded. How could a regional medical center that delivered babies and performed all types of surgery not have platelets on hand for an emergency? Vaclavik called the Red Cross and other facilities, pleading with them to send any they had. “In my understanding, there was a complete shortage of platelets in the state of New Jersey,” he said in the deposition. Hours passed before the needed platelets arrived.
The neuro team did another CT scan around 6 a.m. Larry couldn’t bring himself to look at it, “but from what they’ve told me, it was horrifically worse.” While Lauren was in surgery, friends began dropping by, hoping to see her and the baby, not realizing what had happened since her cheerful texts the night before. Around 12:30 p.m., the neurosurgeon emerged and confirmed that brain activity had stopped. Lauren was on life support, with no chance of recovery.
All this time, Hailey had been in the newborn nursery, being tended by Lauren’s stunned colleagues. They brought her down to Lauren’s room and Larry placed her gently into her mother’s arms. After a few minutes, the nurses whisked the baby back up to the third floor to protect her from germs. A respiratory therapist carefully removed the breathing tube from Lauren’s mouth. At 3:08 p.m., surrounded by her loved ones, she died.
A private tragedy
In the U.S., unlike some other developed countries, maternal deaths are treated as a private tragedy rather than as a public health catastrophe. A death in childbirth may be mourned on Facebook or memorialized on GoFundMe, but it is rarely reported in the news. Most obituaries, Lauren’s included, don’t mention how a mother died.
Lauren’s passing was more public than most, eliciting an outpouring of grief. Hundreds of people attended her wake and funeral — doctors and nurses from the hospital, friends from around the country, families Lauren had taken care of. Vaclavik was there, utterly devastated, Larry’s family said. The head of Monmouth’s ob/gyn department paid his respects and, according to Larry, promised in a private conversation at the wake to conduct a full investigation.
Hailey, now 5, at her mother’s grave. Courtesy of the Bloomstein Family
In the days after Lauren’s death, Larry couldn’t dwell on the implications of what had happened. He had to find a burial plot, choose a casket, write a eulogy. He was too shattered to return to the Mooresville house, so he took Hailey to his parents’ place, a one-bedroom apartment they were renting while they renovated their home, and slept with the baby in the living room for the first month.
After the funeral, he turned all his attention to his daughter. He knew nothing about newborns, always imagining Lauren would teach him — “What could be better than having your own NICU nurse to take care of your baby?” he had thought. He relied on his mother and sister and Lauren’s friends to guide him. He took time off from his job at Cooper, figuring three months would be enough. But as his return date approached, he knew he wasn’t ready. “I don’t think I can see a patient that’s on a ventilator right now,” he realized. “Or even just a hospital bed.” He didn’t want to leave Hailey. So he quit.
He sold the house, though he couldn’t bring himself to attend the closing — “I couldn’t stand handing those keys over to someone else.” He took Hailey a couple of times to stay with his sister and her family in Texas, where he didn’t have to answer the constant questions. But traveling with his baby daughter was painful in its own way. People didn’t know what to make of him. “It’s strange for people to see a father alone,” he said.
Wherever he went, he felt disconnected from almost everything around him: “You’re walking around this world and all these people are around you, and they’re going on with their lives and I just felt very, very isolated and very alone with that.”
Back in New Jersey, Larry found a job closer to his parents’ place, performed one operation and tried to quit. His new employers, though, persuaded him to stay. To avoid reliving the funeral, he returned to Texas for the first anniversary of Hailey’s birth and Lauren’s death in late September 2012. In one of his suitcases, he packed a giant cupcake mold Lauren had bought when they first married — she thought it would make a perfect first birthday cake for the kids she yearned for. He baked the cake himself — chocolate, Lauren’s favorite, covered with sprinkles.
“With our technology, every single time a woman dies, it’s a medical error”
Other people in Lauren’s and Larry’s circle had been asking questions about her care since the night she died. “That was the first thing I literally said when I walked [into the hospital] — I said, ‘How did this happen?'” Jackie Ennis recalled. In the next week or two, she probed Larry again: “‘Did they do everything they could for her?'” He said, ‘No, there were warning signs for hours before.'” Ennis was too upset to dig any deeper.
As Larry’s numbness wore off, his orthopedist friends began pushing him as well. Larry was hesitant; despite the missteps he had witnessed, part of him wanted to believe that Lauren’s death had been unavoidable. “And my friends were like, ‘We can’t accept that … With our technology, every single time a woman dies [in childbirth], it’s a medical error.'”
Lauren’s death, Larry finally admitted to himself, could not be dismissed as either inevitable or a fluke. He had seen how Lauren’s ob/gyn and nurses had failed to recognize a textbook case of one of the most common complications of pregnancy — not once, but repeatedly over two days. To Larry, the fact that someone with Lauren’s advantages could die so needlessly was symptomatic of a bigger problem. By some measures, New Jersey had one of the highest maternal mortality rates in the U.S. He wanted authorities to get to the root of it — to push the people and institutions that were at fault to change.
That’s the approach in the United Kingdom, where maternal deaths are regarded as systems failures. A national committee of experts scrutinizes every death of a woman from pregnancy or childbirth complications, collecting medical records and assessments from caregivers, conducting rigorous analyses of the data, and publishing reports that help set policy for hospitals throughout the country. Coroners also sometimes hold public inquests, forcing hospitals and their staffs to answer for their mistakes. The U.K. process is largely responsible for the stunning reduction in preeclampsia deaths in Britain, the committee noted its 2016 report — “a clear success story” that it hoped to repeat “across other medical and mental health causes of maternal death.”
The U.S. has no comparable federal effort. Instead, maternal mortality reviews are left up to states. As of this spring, 26 states (and one city, Philadelphia) had a well-established process in place; another five states had committees that were less than a year old. In almost every case, resources are tight, the reviews take years, and the findings get little attention. A bipartisan bill in Congress, the Preventing Maternal Deaths Act of 2017, would authorize funding for states to establish review panels or improve their processes.
New Jersey’s review team, the second-oldest in the U.S., includes ob/gyns, nurses, mental health specialists, medical examiners, even a nutritionist. Using vital records and other reports, they identify every woman in New Jersey who died within a year of pregnancy or childbirth, from any cause, then review medical and other records to determine whether the death was “pregnancy-related” or not. Every few years, the committee publishes a report, focusing on things like the race and age of the mothers who died, the causes of death, and other demographic and health data. In the past, the findings have been used to promote policies to reduce postpartum depression.
But the New Jersey committee doesn’t interview the relatives of the deceased, nor does it assess whether a death was preventable. Moreover, like every other state that conducts such reviews, New Jersey “de-identifies” the records — strips them of any information that might point to an individual hospital or a particular woman. Otherwise, the medical community and lawmakers would refuse to go along. The goal is to “improve care for patients in general,” said Joseph Apuzzio, a professor of obstetrics and gynecology at Rutgers-New Jersey Medical School who heads the committee. This requires a process that is “nonjudgmental” and “not punitive,” he said. “That’s the best way to get a free discussion of all of the health care providers who are in the room.”
Yet the result of de-identification, as Larry soon realized, is that the review is of little use in assigning responsibility for individual deaths, or evaluating whether some hospitals, doctors or nurses are more prone to error than others. To Larry, this seemed like a critical oversight — or perhaps, willful denial. In a preventable death or other medical error, he said, sometimes the who and the where are as important as the why. “Unless someone points the finger specifically,” he said, “I think the actual cause [of the problem] is lost.”
“The facility is not in compliance”
Someone eventually steered Larry toward the New Jersey Department of Health’s licensing and inspection division, which oversees hospital and nursing-home safety. He filed a complaint against Monmouth Medical Center in 2012.
The DOH examined Lauren’s records, interviewed her caregivers and scrutinized Monmouth’s policies and practices. In December 2012 it issued a report that backed up everything Larry had seen first-hand. “There is no record in the medical record that the Registered Nurse notified [the ob/gyn] of the elevated blood pressures of patient prior to delivery,” investigators found. And: “There is no evidence in the medical record of further evaluation and surveillance of patient from [the ob/gyn] prior to delivery.” And: “There was no evidence in the medical record that the elevated blood pressures were addressed by [the ob/gyn] until after the Code Stroke was called.”
The report faulted the hospital. “The facility is not in compliance” with New Jersey hospital licensing standards, it concluded. “The facility failed to ensure that recommended obstetrics guidelines are adhered to by staff.”
To address these criticisms, Monmouth Medical Center had implemented a plan of correction, also contained in the report. The plan called for a mandatory educational program for all labor and delivery nurses about preeclampsia and HELLP syndrome; staff training in Advance Life Support Obstetrics and Critical Care Obstetrics; and more training on the use of evidence-based methods to assess patients and improve communications between caregivers.
Some of the changes were strikingly basic: “Staff nurses were educated regarding the necessity of reviewing, when available, or obtaining the patients [sic] prenatal records. Education identified that they must make a comparison of the prenatal blood pressure against the initial admission blood pressure.” And: “Repeat vital signs will be obtained every 4 hours at a minimum.”
An important part of the plan of correction involved Vaclavik, though neither he nor the nurses were identified by name. The head of Monmouth’s ob/gyn department provided “professional remediation for the identified physician,” the Department of Health report said. In addition, there was “monitoring of 100% of records for physician of record per month x 3 months.” The monitoring focused on “compliance of timely physician intervention for elevated blood pressures/pain assessment and management.”
The department chairman, Robert Graebe, found Vaclavik’s charts to be 100 percent compliant, Vaclavik said in the deposition. Graebe was asked in a March 2017 deposition if Vaclavik was in good standing at the hospital at the time of Lauren’s treatment. “Was and is,” Graebe replied.
In a separate note, the Department of Health told Larry that it forwarded his complaint to the Board of Medical Examiners and the New Jersey Board of Nursing. Neither agency has taken disciplinary action, according to their websites.
Larry’s copy of the DOH report arrived in the mail. He was gratified by the findings but dismayed that they weren’t publicly posted. That meant hardly anyone would see them.
A few months after the DOH weighed in, he sued Monmouth, Vaclavik and five nurses in Monmouth County Superior Court in Freehold, N.J. For a medical malpractice lawsuit to go forward in New Jersey, an expert must certify that it has merit. Larry’s passed muster with an ob-gyn. But beyond the taking of depositions, there’s been little action in the case.
Creating “toolkits”
As the maternal death rate has mounted around the U.S., a small cadre of reformers has mobilized. Some of the earliest and most important work has come in California, where more babies are born than in any other state —500,000 a year, one-eighth of the U.S. total.
Modeled on the U.K. process, the California Maternal Quality Care Collaborative is informed by the experiences of founder Elliott Main, a professor of obstetrics and gynecology at Stanford and the University of California-San Francisco, who for many years ran the ob/gyn department at a San Francisco hospital. “One of my saddest moments as an obstetrician was a woman with severe preeclampsia that we thought we had done everything correct, who still had a major stroke and we could not save her,” he said recently. That loss has weighed on him for 20 years. “When you’ve had a maternal death, you remember it for the rest of your life. All the details.”
Launched a decade ago, CMQCC aims to reduce not only mortality but also life-threatening complications and racial disparities in obstetric care. It began by analyzing maternal deaths in the state over several years; in almost every case, it discovered, there was “at least some chance to alter the outcome.” The most preventable deaths were from hemorrhage (70 percent) and preeclampsia (60 percent).
Main and his colleagues then began creating a series of “toolkits” to help doctors and nurses improve their handling of emergencies. The first one, targeting obstetric bleeding, recommended things like “hemorrhage carts” for storing medications and supplies, crisis protocols for massive transfusions, and regular training and drills. Instead of the common practice of “eye-balling” blood loss, which often leads to underestimating the seriousness of a hemorrhage and delaying treatment, nurses learned to collect and weigh postpartum blood to get precise measurements.
Hospitals that adopted the toolkit saw a 21 percent decrease in near deaths from maternal bleeding in the first year; hospitals that didn’t use the protocol had a 1.2 percent reduction. By 2013, according to Main, maternal deaths in California fell to around 7 per 100,000 births, similar to the numbers in Canada, France and the Netherlands – a dramatic counter to the trends in other parts of the U.S.
“Prevention isn’t a magic pill,” Main said. “It’s actually teamwork [and having] a structured, organized, standardized approach” to care.
CMQCC’s preeclampsia toolkit, launched in 2014, emphasized the kind of practices that might have saved Lauren Bloomstein: careful monitoring of blood pressure and early and aggressive treatment with magnesium sulfate and anti-hypertensive medications. Data on its effectiveness hasn’t been published.
The collaborative’s work has inspired ACOG and advocates in a few states to create their own initiatives. Much of the funding has come from a 10-year, $500 million maternal health initiative by Merck, the pharmaceutical giant. Originally intended to focus on less developed countries, Merck for Mothers decided it couldn’t ignore the growing problem in the U.S. The U.S. maternal mortality rate is “unacceptable,” said executive director Mary-Ann Etiebet. Making pregnancy and childbirth safer “will not only save women’s lives but will improve and strengthen our health systems … for all.”
But the really hard work is only beginning. According to the Institute of Medicine, it takes an average of 17 years for a new medical protocol to be widely adopted. Even in California, half of the 250 hospitals that deliver babies still aren’t using the toolkits, said Main, who largely blames inertia.
In New York State, some hospitals have questioned the need for what they call “cookbook medicine,” said Columbia’sD’Alton.. Her response: “Variability is the enemy of safety. Rather than have 10 different approaches to obstetric hemorrhage or treatment of hypertension, choose one or two and make it consistent … When we do things in a standardized way, we have better outcomes.”
One big hurdle: training. Another: money. Smaller providers, in particular, may not see the point. “It’s very hard to get a hospital to provide resources to change something that they don’t see as a problem,” ACOG’s Barbara Levy said. “If they haven’t had a maternal death because they only deliver 500 babies a year, how many years is it going to be before they see a severe problem? It may be 10 years.”
In New Jersey, providers don’t need as much convincing, thanks to a recent project to reduce postpartum blood loss led by the Association of Women’s Health, Obstetric and Neonatal Nurses. A number of hospitals saw improvements; at one, the average length of a hemorrhage-related ICU stay plunged from 8 days to 1.5 days. But only 31 of the state’s 52 birthing hospitals participated in the effort, in part — perhaps — because nurses led it, said Robyn D’Oria, executive director of the Central Jersey Family Health Consortium and member of the state’s maternal mortality committee. “I remember having a conversation with [someone from] a hospital that I would describe as progressive and she said to me, ‘I cannot get past some of the physicians not wanting to buy into this.'”
So New Jersey hospitals are about to try again, this time adopting mini-toolkits created by the ACOG-led Alliance for Innovation on Maternal Health for hemorrhage and preeclampsia. “We’re at the very beginning” of a roll-out that is likely to take at least two years, D’Oria said. Among those helping create momentum has been Ryan Hansen, the husband of the teacher who died at Monmouth Medical Center a few months before Lauren Bloomstein.
Larry and Carolyn Bloomstein play with their daughters Aria, 2, (left) and Hailey, 5, at home in New Jersey. Bryan Anselm for ProPublica
Still, as hospitals begin to revamp, mothers in the state continue to perish. One was Ashley Heaney Butler. A Rutgers University graduate, she lived in Bayville, where she decorated the walls of her house with anchors, reflecting her passion for the ocean. She worked for the state Division of Vocational Rehabilitation Services as a counselor and served as president of the New Jersey Rehabilitation Association. Her husband Joseph was a firefighter. She gave birth at Monmouth last September to a healthy boy and died a couple of weeks later at the age of 31, never leaving the hospital. It turned out that she had developed an infection late in her pregnancy, possibly related to a prior gastric bypass surgery. She was under the care of several doctors, including Vaclavik.
“She didn’t get what she deserved”
The sudden death of a new mother is tragic to everyone around her. “When you take that one death and what that does, not only to the husband but to the family and to the community, the impact that it has in the hospital, on the staff, on everybody that’s cared for her, on all the people who knew them, it has ripple effects for generations to come,” Robyn D’Oria said.
Jackie Ennis felt Lauren’s loss as an absence of phone calls. She and Lauren had been closer than many sisters, talking several times a day. Sometimes Lauren called just to say she was really tired and would talk later; she’d even called Ennis from Hawaii on her honeymoon. The night Lauren died, Ennis knew something was wrong because she hadn’t heard from her best friend. “It took me a really long time not to get the phone calls,” she said. “I still have trouble with that.”
During Lauren’s pregnancy, Frankie Hedges had thought of herself as Hailey’s other grandmother. She and Lauren had made a lot of plans. Lauren’s death meant the loss of their shared dreams for an entire extended family. “I just feel she didn’t get what she deserved,” Hedges said.
Vaclavik’s obstetric practice is “larger” than in 2011, and he continues to have admitting privileges at Monmouth and two other hospitals, he said in his deposition. “I will never forget” Lauren’s death, he said. “… I probably suffer some post traumatic stress from this.”
Hailey is five years old, with Lauren’s brown hair and clear green eyes. She feels her mother’s presence everywhere, thanks to Larry and his new wife Carolyn, whom he married in 2014. They met when she was a surgical tech at one of the hospitals he worked at after Lauren died. Photos and drawings of Lauren occupy the mantle of their home in Holmdel, the bookcase in the dining room, and the walls of the upstairs hallway. Larry and Carolyn and their other family members talk about Lauren freely, and even Larry’s younger daughter, 2-year-old Aria, calls her “Mommy Lauren.”
On birthdays and holidays, Larry takes the girls to the cemetery. He designed the gravestone — his handprint and Lauren’s reaching away from each other, newborn Hailey’s linking them forever. Larry has done his best to keep Lauren’s extended family together— Ennis and Hedges and their families are included in every important celebration.
Larry still has the video of Lauren and Hailey on his phone. “By far the hardest thing for me to accept is [what happened] from Lauren’s perspective,” he said one recent evening, hitting the play button and seeing her alive once more. “I can’t, I literally can’t accept it. The amount of pain she must have experienced in that exact moment when she finally had this little girl … I can accept the amount of pain I have been dealt,” he went on, watching Lauren stroke Hailey’s cheek. “But [her pain] is the one thing I just can’t accept. I can’t understand, I can’t fathom it.”
NPR’s Bo Erickson, and ProPublica’s research editor Derek Kravitz and engagement reporter Adriana Gallardo contributed to this report.
Copyright 2017 NPR. To see more, visit http://www.npr.org/.
After assembling suicide bomb vests for the attacks that slaughtered 130 people in Paris last November, Najim Laachroui went underground in his native Brussels.
The 24-year-old explosives expert wasn’t just hiding from the biggest manhunt in Europe’s recent history. He was plotting. In a dingy apartment converted into a bomb factory, Laachroui exchanged a series of messages in French with Abu Ahmed, a shadowy commander in the Islamic State based in Syria.
If law enforcement agencies had intercepted the communications, they would have been immediately alarmed. Laachroui asked militants in Syria to test chemical mixtures so he could assemble powerful bombs. He discussed his hopes to strike France again and disrupt a soccer championship there. He reported that he and half a dozen other fugitives from the Paris attacks had split up among three safe houses, according to Belgian and French counterterror officials.
Although U.S and European spy agencies were scouring the internet for any trace of Laachroui, they failed to intercept those exchanges. The reason, U.S. and European counterterror officials say: during Laachroui’s four months on the run, he and Abu Ahmed communicated through Telegram, an encrypted messaging application, and other widely available tools for secure communications.
On March 15, Belgian police raided a safe house and killed another leader of the terrorist cell in a gunfight. A worried Laachroui sent a message to Abu Ahmed reporting that the raid had cost the plotters the stash of ammunition for their AK-47 rifles, according to Belgian and French counterterror officials.
“The original plan at the airport was for them to do an attack more like Paris: shoot a lot of people first, and then set off the bombs,” a Belgian counterterror official explained in an interview in April. “But they didn’t have ammo because it was left behind in the safe house. Laachroui says: ‘We don’t have chargers for our guns. What do we do?’ They were told to go ahead and attack just with bombs’.”
On March 22, they did just that. Laachroui and two other suicide bombers killed 32 people at the airport and at a subway station in Brussels. Afterward, investigators found a laptop computer that helped them reconstruct Laachroui’s encrypted audio and text exchanges with his commander in Syria, according to European counterterror officials.
The communications were described by European and U.S. counterterror officials to ProPublica, which is preparing a documentary about terrorism in Europe in collaboration with the PBS program Frontline. ProPublica interviewed counterterror officials in Europe and the United States, some on condition of anonymity, and reviewed intercepted conversations documented in European court cases.
Taken together, the voices of the Islamic State offer insights into the day-to-day workings of an organization that has carried out lethal attacks in Baghdad, Bangladesh, and Turkey in the past two weeks.
The culture of ISIS mixes the centralized control that characterized al-Qaida with a more freewheeling approach that gives its operatives considerable latitude. The group’s use of digital propaganda to inspire “self-radicalizing” terrorists has drawn attention with attacks on U.S. soil in San Bernardino and Orlando. But the communications collected in Europe show the group provides direct long-distance instructions to operatives it dispatches from its base in Syria, and they rely heavily on that guidance.
The European communications also clearly establish the importance of encryption to ISIS operations.
“We are dealing with a challenge right now: New technologies that enable encryption and allow them to be fairly confident that they are communicating in a way that can’t be detected,” a senior U.S. intelligence official said. “They know how to communicate securely. Often we are inhibited: We know the fact of the communications taking place without knowing the content.”
In April, Italian police overheard a senior figure in Syria urging a Moroccan suspect living near Milan to carry out an attack in Italy, according to a transcript. Although the voice message had been sent through an encrypted channel, the Moroccan played it back in his car, where a hidden microphone recorded it.
In the message, the unidentified “sheik” declared: “Detonate your belt in the crowds declaring Allah Akbar! Strike! (Explode!) Like a volcano, shake the infidels, confront the throng of the enemy, roaring like lightning, declare Allah Akbar and blow yourself up, O lion!”
The suspects exchanged recorded messages over WhatsApp, an encrypted telephone application that is widely used in Europe, the Arab world and Latin America. FBI Director James Comey and other counterterror officials have publicly expressed concern about extremists in the United States using such techniques to elude monitoring.
“We’ll be monitoring a couple of guys in an internet chatroom,” a former FBI counterterror official said in an interview. “Then you’ll see one of them says: OK, reach out to me on WhatsApp.’ At that point, we can’t do anything.”
Executives at WhatsApp and Telegram defend encryption as a vital shield to privacy. Reached for comment last week, a spokesperson at WhatsApp said the company complies with U.S. laws requiring cooperation with law enforcement agencies. The spokesperson cited a statement by executives in April when WhatsApp implemented “end-to-end” encryption that will conceal the content of users’ communications even from the company itself.
“Encryption is one of the most important tools governments, companies, and individuals have to promote safety and security in the new digital age,” said Jan Koum, the company’s founder, in a blog post in April. “While we recognize the important work of law enforcement in keeping people safe, efforts to weaken encryption risk exposing people’s information to abuse from cybercriminals, hackers, and rogue states.”
(Facebook, which owns WhatsApp, announced Friday that it would add end-to-end encryption for some photo and text messages on its Messenger application.)
Telegram did not respond to a request for comment for this article last week. But company executives have publicly addressed concerns about encryption by saying that technology comes with an inevitable dark side. The company says it has shut down more than 660 public channels on its application that were being used by the Islamic State.
Intelligence officials say the Islamic State’s failure to launch Paris-style attacks in the United States reflects differences in both geography and demography. American Muslims are less radicalized and less numerous than those in Europe, and U.S. border security makes it harder for would-be terrorists to enter the country, according to Western counterterror officials.
In Europe, the Islamic State has found support in large and restive Muslim communities, especially among criminals who radicalize more rapidly today than previous generations of hoodlums-turned-jihadis. Investigators say intensified Western military pressure in Iraq and Syria has prompted the group to order European recruits to strike immediately rather than make the pilgrimage to the caliphate.
“In the context of the current strategy of the Islamic State, it’s clear that their focus is causing casualties here,” said Claudio Galzerano, commander of a counterterrorism unit of the Italian police.
The ISIS strategy toward the West has evolved since the Islamic State conquered a swath of territory in Syria and Iraq and declared the caliphate two years ago, causing thousands of militants to flock to Syria.
Previous generations of aspiring jihadis passed through a series of filters as they journeyed to al-Qaida training camps in South Asia, often with a first stop at radical mosques in London. This selective, secretive approach allowed al-Qaida to vet prospective holy warriors and detect attempts at infiltration by intelligence services.
In contrast, the flow to Syria has been larger, faster and less security-conscious. Taking advantage of Europe’s proximity and ease of travel, fighters who rushed to Syria posted photos of themselves online brandishing guns. Their ranks included criminals and thrill-seekers with little religious knowledge, according to Marc Trevidic, a veteran French counterterror judge.
The Islamic State “has accepted for strategic reasons, because it wanted to impose itself on other groups in the region, the recruitment of anyone,” Trevidic said. “Methods will be created afterwards to check that … they are not spies, etcetera, but initially there are no filters.”
An Italian investigation begun in 2014 documented that hectic period. Tracking jihadis from Italy, police intercepted the cell phones of senior figures in Turkey and Syria, according to a 44-page report by a Milan investigative magistrate dated June 12, 2015. A Turkish phone was used primarily by Ahmed Abu al Harith, “a significant member of the terrorist organization with the role … of coordinating volunteers arriving in Turkey and headed to join the Islamic State,” the report says.
Monitored in late 2014 and early 2015, Ahmed Abu al Harith and fellow coordinators spoke multiple languages with callers from 22 countries including Afghanistan, Saudi Arabia, Georgia, San Marino and Sweden.
They explained “concrete rules for joining the Islamic State already described on the internet in a manual titled ‘Hijrah [Pilgrimage] to the Islamic State 2014 what to bring, whom to contact, where to go’,” according to the Italian report.
The coordinators didn’t use encryption or coded language. But they banned recruits from traveling with “latest-generation mobile devices” in order to “avoid being located” by spy agencies. The Islamic State wanted recruits to leave behind smartphones, tablets and other devices with existing trails of activity that make them easier to trace, and use new, disposable cell phones instead, the report says.
Some recruits were less than sophisticated about the directives.
On Jan. 4, 2015, an exasperated coordinator repeatedly explained to a befuddled caller with a Lebanese accent that he could only bring a basic cell phone to Syria, according to a transcript.
“The important thing is that when you arrive in Turkey you have a small cell phone to contact me,” the coordinator said. “Don’t bring smart phones or tablets. OK, brother?”
For the fourth time, the recruit asked: “So we can’t have cell phones?”
“Brother, I said smart phones: iPhone, Galaxy, laptop, tablet, etcetera.”
Sounding a bit like a frustrated gate agent at a crowded airport, the coordinator added: “Each of you can only bring one suitcase. If you come alone, just bring one suitcase. That is, a carry-on and one suitcase.”
“I didn’t understand the last thing, could you explain?”
“Brother, call me when you get to Turkey.”
In Syria, new arrivals were interviewed by Islamic State militants seated at computers, according to Western counterterror officials. The militants asked a checklist of questions including blood type, mother’s name, level of religious education, and preference for becoming a “warrior” or a “martyr,” according to copies of Islamic State intake forms obtained by ProPublica. The authenticity of the documents was confirmed by U.S. counterterror officials.
Although the culture of the Islamic State is repressive and bureaucratic, the reality on the ground can be rather anarchic. The restrictions on high-tech devices described in the Italian investigation were by no means uniformly imposed or obeyed. Militants in the self-styled caliphate have access to computers, smart phones and social media. Some have posted a barrage of messages and images, including videos of atrocities.
In response, leaders of the Islamic State have told foreign fighters to curtail their activity on social media because it exposes them to eventual prosecution back home or to being targeted in Syria. The use of social media has continued, however, according to European counterterror officials.
In fact, the cacophony of voices from Syria has been crucial to recruitment.
“In contrast to what has happened with other conflicts, the recruitment and the propaganda aren’t just in hands of the public communications apparatus,” said a counterterror chief of the Spanish police. “Each fighter has a phone and narrates his day-to-day life, his blog … A lot of these terrorists have circles of associates in Europe because they came from there, so this is effective publicity.”
Tapping into such communications, Italian police gained insight from their investigation of a family of Muslim converts from the Milanese suburb of Inzago.
Maria Giulia Sergio was 28. In September of 2014, she married an Albanian extremist she barely knew so they could join the Islamic State, according to investigators. The couple traveled with his mother to the Syrian city of Sed Forouk and met up with Albanian relatives living there, including children. The husband’s brother died in combat, according to the report.
The newlyweds encountered “numerous daily obstacles” to staying in touch with people back home because of “rigid rules imposed by the Islamic State as well as the objective technical difficulties, in a country devastated by years of civil war,” the report says. “This had a positive impact on the investigations because it had the practical effect of multiplying calls among relatives” in Italy and Albania when they heard from the militants.
Sergio talked via Skype because the suspects believed it was “more secure,” the report says. Police intercepted the conversations nonetheless. Sergio described her husband’s stint in a training camp in Iraq. She talked about child care, Koranic classes, decapitations and a stoning, and implored her family to make the “hijrah,” or pilgrimage to Syria.
“I am speaking to you in the name of the Islamic State,” she said. Scolding her father for remaining in his job in Italy, she said: “It makes no sense for you to work for them. They are the ones who must be our slaves.”
In April of last year, the parents announced they would join her. The father asked if he should bring his driver’s license and if he could buy a car in the “Caliphate,” according to the transcript.
Police arrested the suspects before they could depart.
Meanwhile, authorities across Europe struggled to intercept a smaller flow of militants traveling in the opposite direction.
Western intelligence officials estimate that the Islamic State dispatched between 60 and 180 operatives to attack targets in Europe. The strategy appears to have been to overwhelm the security forces with sheer numbers. Even if most of the strikes failed, something would eventually succeed. The results were graphically evident in France, where authorities foiled 11 attacks in 2015.
Officials say the threat has changed since the days of al-Qaida. Osama bin Laden’s group had the flexibility common to Islamist terror networks, often developing plots based on the initiative, expertise and availability of recruits who reached its secret compounds in Afghanistan and Pakistan.
Al-Qaida created a team to oversee attacks overseas. The chief plotters were Middle Easterners or Pakistanis, and they guided operatives to targets with instructions via phone and email. U.S. counterterror agencies identified external operations chiefs and eliminated a series of them with drone strikes and captures.
Today, the counterterror community is still mapping out the Islamic State’s leadership, especially those involved in foreign plots, according to the senior U.S. intelligence official.
“The structure that promotes attacks is wider and deeper, but to some degree also more autonomous, than what we saw with al-Qaida,” the official said. “It isn’t the case where we can home in on individuals and have a fair degree of confidence that if we neutralize them we will have had a considerable impact on the threat. That’s not the situation with ISIS. We had a fairly comprehensive view of the structure of al-Qaida … With ISIS, we don’t have an exact picture. It’s an intelligence collection challenge that we are working hard to address.”
The Islamic State’s top echelons are dominated by Gulf Arabs, Syrians and Iraqis, including former military and intelligence officers. Foreign fighters serve in units known as “katibas” organized by nationality and language. Large Francophone katibas field hundreds of French and Belgians, many of North African descent, and thousands of Moroccans and Tunisians. Senior foreign fighters have the resources of a quasi-state at their disposal: money, technology, identity documents, training facilities. But they are also given considerable autonomy to develop plots, officials say.
“There is … leeway to foreign fighters and operatives to choose targets and methods on turf they know best,” the senior U.S. intelligence official said. “The foreign fighters know what the organization wants to see happen and they act on it.”
The attacks on Paris in November briefly made Abdelhamid Abaaoud, a 28-year-old Belgian ex-convict, an internationally known leader of the external operations unit. He participated in the massacre and died in a police raid days later in the gritty suburb of Saint Denis. Yet some investigators now believe his stature within the Islamic State has been overstated.
“To me he was an average leader,” said Judge Trevidic, who led investigations of plots in which Abaaoud surfaced. “Have you ever seen a general on the front in Saint Denis? That is all right for a lieutenant, a captain, but not for people above. 2018′
Based in Syria, Abaaoud selected, trained and deployed jihadis to Europe in 2014 and the first half of 2015. In addition to guns and grenades, he taught trainees about secure communications 2014 encrypted applications such as Telegram, WhatsApp and Truecrypt 2014 and set up protocols to contact them when they were in place.
Secure communications technology has been a recurring feature in recent attacks and foiled plots in France, according to French Interior Minister Bernard Cazenueve.
“Encryption is a crucial issue,” Cazeneuve told a small group of U.S. reporters in March. “All the attacks last year used encrypted phones or computers … It is a difficult problem for us.”
(For background on the use of encryption by terrorists, read this article in the June issue of The CTC Sentinel, the monthly publication of the Combating Terrorism Center at West Point.)
Abaaoud’s operatives did not always follow security procedures, however. In June of last year, Turkish immigration authorities detained Tyler Vilus, a French plotter en route to Paris with someone else’s Swedish passport. Allowed to keep his cellular phone in a low-security detention center, Vilus brazenly sent an unencrypted text message to Abaaoud in Syria, according to a senior French counterterror official.
“I have been detained but it doesn’t seem too bad,” the message said, according to the senior official. “I will probably be released and will be able to continue the mission.”
Instead, U.S. spy agencies helped retrieve that text and French prosecutors charged Vilus with terrorist conspiracy.
In another case linked to Abaaoud in early 2014, the NSA played a central role in helping French police track down Ibrahim Boudinah, a plotter captured in a Cannes safe house as he prepared an attack with explosives and guns.
Officials said the Paris plot did not involve much long-distance direction. Instead, Abaaoud and two other field coordinators travelled separately from Syria to Europe to prepare the attack. Abaaoud entered via Greece in September, probably melting into a vast, chaotic flow of illegal immigrants that the Islamic State has used to infiltrate operatives during the past two years.
The other two leaders made their way to Budapest, where they sheltered in crowds of refugees camped out in the train station, according to Belgian prosecutors. On September 9, they were picked up at the train station by a Belgian accomplice named Saleh Abdeslam, who drove them to Belgium, prosecutors say.
The pair had different skills. Laachroui, a former electrical engineering student from Brussels, was the explosives expert. Belkaid, an Algerian petty criminal who lived in Sweden before joining the Islamic State, had more ideological preparation and religious knowledge than the others in the attack squad, officials say.
In Brussels, the duo set up a remote command post in a safe house and coordinated the Paris operation by phone. The gunmen and bombers used a number of disposable cell phones during the attacks. Although police reconstructed the activity of a phone found near the scene of the attack on the Bataclan concert hall, plotters exchanged encrypted messages before the attacks that French intelligence could not detect, according to Interior Minister Cazenueve.
Afterward, the coordinators in Brussels made calls and wired money to help Abaaoud, who was on the run, rent the shabby apartment north of Paris where police eventually killed him. Intercepted calls suggested that Laachroui and Belkaid “had some rank or influence,” a senior Belgian counterterror official said.
Laachroui and Belkaid became targets of a massive manhunt along with Abdeslam, the lone surviving attacker from Paris, and several other accomplices. They were sheltered for four months in Brussels by networks based on clan, ethnicity and criminality and ruled by a code of silence. Police monitored at least 89 phones. An intercept picked up ominous chatter.
“It was possibly Saleh [Abdeslam] or an associate,” the Belgian counterterror official said. “He’s saying: ‘The cops are chasing me. Things are hot here. We are going into action.’ And the voice in Syria says: ‘Yes, go into action.’ But there wasn’t intelligence of a precise plan.”
That snippet of intelligence was among the leads that prompted Belgian authorities to shut down their capital for five days in November. But the attack didn’t happen for a while.
During the next four months, the bombmaker Laachroui stayed in close contact with the Islamic State using encrypted methods, principally Telegram, according to Western counterterror officials. The fugitives also communicated with Syria and each other using WhatsApp, Skype and the mobile application Viber on devices including laptops, tablets and phones, counterterror officials said.
Laachroui exchanged audio recordings and text messages with Abu Ahmed, a French-speaking “emir” of foreign fighters in Syria, counterterror officials said. Investigators believe Abu Ahmed was based in Raqqah, the Islamic State’s headquarters, and that he also played a role in overseeing the Paris plot.
It’s not clear if Western intelligence officials have identified Abu Ahmed yet. Several veteran French jihadis in Syria are suspected of overseeing external operations. They include the converts Fabien and Jean-Michel Clain, brothers from Toulouse (Fabien Clain is believed to have issued the Islamic State’s claim of responsibility for the Paris attacks); Boubaker el Hakim and Salim Benghalem, Parisian veterans of a cell that first waged jihad in Iraq in 2004; and a blond convert known as Abu Sulayman al Fransi, described as a former physical education teacher and father of two.
At one point, Laachroui told Abu Ahmed there were tensions among the fugitives in Brussels, according to officials.
“They were squabbling,” the Belgian counterterror official said. “They told the emir: ‘We have split up. We were arguing before. It’s better now.'”
As Laachroui worked with TATP, a highly volatile explosive, in his hideout in the Schaarbeck neighborhood, he asked Abu Ahmed for technical help from bomb experts in Syria.
“He has them check different mixtures and adjusts his work based on what they tell him,” the Belgian counterterror official said.
The fugitives and the emir discussed potential plans including a massive attack with 600 kilos of explosives that did not take place. The goal was to wait and strike France again in hopes of disrupting or cancelling the month-long Euro 2016 soccer championship scheduled to begin in June, according to counterterror officials.
European spy agencies and their allies in the United States and Britain deployed the full weight of their sophisticated technology in the search for the plotters. But neither the NSA nor Britain’s Government Communications Headquarters (GCHQ), spotted the digital footprints, officials said.
“Everyone was trying to find these guys,” the senior French counterterror official said. “They were able to elude us. But they were able to elude the Americans, too, and that shows you what a problem encryption is.”
Police work on the ground produced a breakthrough on March 15. A forgery investigation turned up fake identity cards used to rent apartments. Police went to what they thought was an abandoned safe house near a Renault factory in the Forest neighborhood.
The raiders used a hand-held battering ram on the door. They discovered Belkaid aiming an AK-47 at them. The firefight wounded him and several investigators, who tumbled down a flight of stairs seeking cover. A SWAT team finished off Belkaid. Police found the cache of ammunition for AK-47 rifles–and DNA traces of Abdeslam, who had fled while Belkaid held off the officers.
The bad news reached Laachrooui, who sent the urgent message to Syria. Abu Ahmed told him just to use bombs, and the fugitives decided to hit Belgium rather than France because time was running out. Once again, the Islamic State let them decide targets and timing, counterterror officials say.
On March 22, Laachroui and another suicide bomber blew up at the Brussels airport. A third bomber struck at a subway station. Thirty-five people died and more than 300 were wounded.
It could have been worse. Two other bombers lost their nerve and fled. The improvised nature of the attack raises the possibility that it might not have succeeded without the guidance from afar.
Airstrikes and battlefield losses have intensified pressure on the Islamic State. It has become more difficult for plotters to enter Europe illegally and for recruits to reach Syria, counterterror officials say.
But terror groups often accelerate attacks abroad in response to defeats at home, as reflected by a recent flurry of strikes in Turkey, Iraq and Bangladesh.
An Italian investigation this year gives glimpses of a changing landscape. The chief suspect was Abderrahim Moutaharrik, a Moroccan immigrant living north of Milan with his wife and two children. A professional kickboxer, he was so radical that he posted a photo of himself in the ring wearing a t-shirt with the Islamic State logo, investigators say.
Moutaharrik and his associates used WhatsApp extensively, according to a 72-page Milan prosecutor’s report dated April 19, 2016. The police secreted microphones in homes and cars and implanted mobile devices with spyware, the report says.
Moutaharrik idolized Mohamed and Osama Koraichi, brothers fighting for the Islamic State. His desire to emulate his friends increased after Osama died in an air strike in Iraq last year. Moutaharrik sang jihadi anthems and ranted about killing infidels in front of his four-year-old son, the report says. His wife obtained a bank loan of $7,800, allegedly to finance their imminent move to Syria.
But there were problems. Mohamed Koraichi was difficult to reach and couldn’t find the family a smuggler in Turkey.
On March 15, Moutaharrik finally received an audio message from Koraichi via WhatsApp from an Indonesian phone in Syria. They discussed the kickboxer’s hopes of making the pilgrimage.
On March 20, Moutaharrik received another WhatsApp message from Syria. But this time a new voice addressed him by name: a high-ranking militant who spoke flowery classical Arabic. He wanted the kickboxer to wage jihad right away.
The “sheik” said the Islamic State was under attack by “Christian” armies from “bases in your homes, European bases,” according to the transcript.
“You must take revenge on them, revenge for the Muslims,” the sheik said. Praising “lone-wolf” operations, he continued: “in the Christian nations, one operation gives more satisfaction than dozens of bombs … You will be among those who do this good deed in the lands of the Christians, in Rome, in Italy …”
“We will take revenge,” Moutaharrik replied, according to the transcript. “God willing here they will only know massacres and killings.”
The police went on red alert. Suicide bombers struck Brussels two days later. Moutaharrik and his wife celebrated, according to transcripts. The sheik and Koraichi urged the increasingly agitated kickboxer to attack right away.
Italy “is the capital of those who carry the cross, my brother,” Koraichi said. “Until now there hasn’t been any operation done [in Italy], know that if you do an attack it is a great thing.”
On April 8, the sheik sent a soliloquy that he titled “Bomb Poem.” It evoked images of fire, suicide bomb belts, and Islamic battalions “annihilating the infidels.”
Police arrested Moutaharrik and three other suspects 11 days later.
ProPublica is a Pulitzer Prize-winning investigative newsroom. Sign up for their newsletter.
Oxycodone 30 mg. (Creative Commons photo by Patrick Ireland)
The overdose death toll from opioids, both prescription drugs and heroin, has almost quadrupled since 1999. In 2014 alone, 28,000 people died of opioid overdoses, more than half from prescription drugs.
Just last month, public awareness of the opioid epidemic reached a new level when Prince was found dead with prescription narcotics on him and authorities began to investigate their role in his demise. In recent weeks, lawmakers and regulators have moved to augment treatment options for addiction and to require more education for doctors who prescribe opioids. The U.S. House of Representatives is voting on a package of bills this week; the Senate passed its own bill in March.
Also in that span, the Los Angeles Times has published an investigation of Purdue Pharma, the maker of the blockbuster pain pill OxyContin, and CNN held a town hall meeting on the consequences of addiction to narcotics. Dr. David A. Kessler, former commissioner of the Food and Drug Administration, wrote an op-ed in the New York Times, calling the embrace of opioids “one of the biggest mistakes in modern medicine.”
Today, ProPublica added warnings labels to the pages of narcotic drugs in our Prescriber Checkup news app, prompted by indications that some readers are using the tool to find doctors who will prescribe these drugs with few or no questions asked (See our editor’s note).
The effectiveness of any of these steps remains to be seen. There is broad consensus on the need for more treatment options, more education, more careful prescribing by doctors. But there’s still much debate about the details—and funding–for each of those steps.
What’s clear is that in recent months there has been an increasing emphasis on the role of health providers and the agencies that oversee them to stem access to widely abused prescription drugs:
In March, the Centers for Disease Control and Prevention released guidelines on prescribing of opioids for chronic pain, defined as pain that lasts for more than three months (excluding pain related to cancer, end-of-life and palliative care.) The guidelines call on doctors to choose therapies other than opioids as their preferred option; to use the lowest possible doses; and to monitor all patients closely.
That same month, the FDA announced tougher warning labels on immediate-release opioids, such as fentanyl, hydrocodone, and oxycodone, to note the “serious risks of misuse, abuse, addiction, overdose and death.”
Nonprofit groups and medical experts in April asked the federal Centers for Medicare and Medicaid Services to remove questions about pain control from a survey of hospital patients’ satisfaction to remove any incentive to overtreat pain. And they asked The Joint Commission, which accredits health facilities, to revise its standards to deemphasize “unnecessary, unhelpful and unsafe pain treatments.” The commission pushed back, saying its standards do no such thing.
Just yesterday, Dr. Steven J. Stack, president of the American Medical Association, called on doctors to do more. He encouraged doctors to use their state’s Prescription Drug Monitoring Program to ensure their patients aren’t shopping for multiple doctors to prescribe them drugs. He called on them to co-prescribe a rescue drug, naloxone, to patients at risk of overdose. And he told them to generally avoid starting opioids for new patients with chronic, non-cancer pain.
“As physicians, we are on the front lines of an opioid epidemic that is crippling communities across the country,” Stack wrote in a statement, published on the Huffington Post. “We must accept and embrace our professional responsibility to treat our patients’ pain without worsening the current crisis. These are actions we must take as physicians individually and collectively to do our part to end this epidemic.”
President Obama during a speech in Cuba. Desmond Boylan/AP
The Obama administration has roundly criticized states such as North Carolina and Mississippi for passing laws that allow discrimination in the name of religious freedom. But at the same time, the administration has left in place a 2007 memo from the Bush White House that allows religious charities with federal contracts to discriminate in hiring for federally funded programs.
Now, as Obama prepares to leave office, a group of prominent constitutional lawyers is calling on the Obama White House to revoke the legal memo, which they argue has been used by religious groups to refuse to provide services, including emergency contraception for human trafficking victims, that conflict with their beliefs. Their arguments are detailed in a legal analysis published this morning by Columbia Law School’s Public Rights/Private Conscience Project, which includes contributions of scholars from George Washington, Emory and Brigham Young universities, among others.
The 16-page paper is, in part, an effort to put pressure on Obama to rescind the memo, an action that does not require Congress to act. As a presidential candidate in 2008, Obama criticized the Bush Justice Department for drafting it, but as president failed to follow through.
“For this administration that has been so strong in so many ways on important civil rights questions and in opposition to similar efforts at the state level to sanction discrimination — to allow this memo to remain in place — is really very unfortunate,” said Ian Thompson, a legislative representative in the American Civil Liberties Union’s Washington, D.C. office. The Columbia paper, he said, is groundbreaking in terms of both its signatories and its scope. “They cover the waterfront in terms of pointing out the dangers and the harms of the memo being in place,” he said.
Bush administration lawyers wrote the memo after the Christian charity World Vision, which serves the poor in nearly 100 countries, objected to a nondiscrimination clause in a $1.5 million Department of Justice grant to fund a mentoring program for at-risk children. World Vision argued that it should be allowed to hire only Christian employees for the program and that not allowing the group to do so would put a “substantial burden” on it.
As justification, the nonprofit cited the 2000 Religious Freedom Restoration Act (RFRA), which bars the government from substantially burdening people’s ability to practice religion unless it has a compelling interest to do so. The Bush White House’s Office of Legal Counsel interpreted the law to mean that World Vision—and by extension, other faith-based organizations—could hire on the basis of faith for federally funded positions.
World Vision argues that withdrawing the memo will only hurt the poor recipients of the charity’s help. “[It] would call into question federal laws and would divert faith-based grantees’ time and funds from serving the needy to litigating to re-clarify the law,” World Vision’s chief legal officer, Steve McFarland, said in a statement.
The Columbia analysis says that since the government is not forcing faith-based organizations to apply for grants, it invalidates the argument that they are being substantially burdened. Instead, the organizations are freely choosing to bid on government contracts with certain conditions specified in advance.
The analysis also highlights examples in which some religious groups have expanded the scope of the 2007 memo, using it as a legal justification to cherry-pick what provisions of a federal grant to fulfill. For example, when the United States Conference of Catholic Bishops (USCCB) won a 2005 grant from the Department of Health and Human Services (HHS) to provide assistance to human trafficking victims, the bishops did not provide contraception or abortion. The ACLU sued HHS in 2009, and the agency ended its contract with the USCCB in 2011.
“The agency is writing the terms of the grant,” said George Washington University Law professor Ira Lupu, who signed the Columbia analysis. Grant applications don’t ask faith-based organizations for their potential objections, and government oversight of grant recipients varies from agency to agency.
In 2014, as unaccompanied children fleeing violence in Central America were held at the U.S.-Mexico border, the Office of Refugee Resettlement drafted guidelines for grant-receiving agencies working with the minors. The proposed rules required caregivers to provide emergency contraception or abortion to children who required it. The USCCB, along with four other faith-based organizations, wrote a letter in February 2015 to the Obama administration to ask for a faith-based exemption to the contraceptive/abortion requirement in the grant rules. The USCCB cited the World Vision Memo in the letter. The Office of Refugee Resettlement hasn’t yet issued finalized rules.
Some legal scholars argue that by keeping the memo in place, the Obama White House is giving ammunition to groups who sue the government in religious liberty cases. . In March, the federal government argued against expanding RFRA in the Supreme Court case Zubikv. Burwell, which centers on just how far to accommodate religious nonprofits that object to the mandate to provide contraception to employees.
“If the inability to receive a grant constitutes a substantial burden on religion, then certainly the requirement to do something would seem to constitute a substantial burden,” said Robert Tuttle, a law professor at George Washington University who signed the Columbia analysis.
The Obama administration has taken steps to address religious discrimination by faith-based organizations. On May 4, new guidelines went into effect that require government agencies to provide a channel for people receiving aid through federal grant programs to report wrongdoing by service providers. The guidelines follow a 2010 executive order—updating a Bush executive order—that prohibits discrimination against aid recipients.
“The Administration has not condoned religious discrimination against beneficiaries of federal aid,” Melissa Rogers, special assistant to the president and executive director of White House Faith-Based and Neighborhood Partnerships, said in an emailed statement, citing the May 4 guidelines and the 2010 executive order. The White House referred direct questions on the World Vision Memo to the Justice Department. The Justice Department and the authors of the memo did not respond to requests for comment.
But, legal experts say, the Obama administration is not doing all it can to protect beneficiaries until the World Vision Memo is rescinded. Katherine Franke, faculty director of the Public Rights/Private Conscious Program at Columbia, said the guidelines put the onus of spotting and reporting wrongdoing on already vulnerable populations.
“What we’re talking about is on one hand general guidance coming from the government and on the other hand a set of legal arguments,” Tuttle said. “So these are government-made legal arguments that lawyers for [grant] recipients can use and say, ‘We know those are your general guidelines, but we are different, and you recognized that in the [World Vision] memo.'”
The Columbia analysis follows several recent high-profile attempts to get the administration to reconsider the memo. Members of Congress wrote to Attorney General Loretta Lynch in February asking for a review and reconsideration of the memo. Advocacy groups wrote letters in 2014 and 2015. Maggie Garrett, legislative director for Americans United for Separation of Church and State, said the groups haven’t received a response.
Just as many organizations have written to the administration asking that it keep the memo in place. University of Virginia School of Law professor Douglas Laycock, who filed a brief with the Supreme Court in favor of the government’s position in Zubik, has assured the administration that the memo is legally sound.
At the very least, the authors of the Columbia analysis hope the administration formally clarifies that the memo only applies to religious hiring — and no more.
“Leaving it in place tarnishes the civil rights record of the Obama administration,” Garrett said.




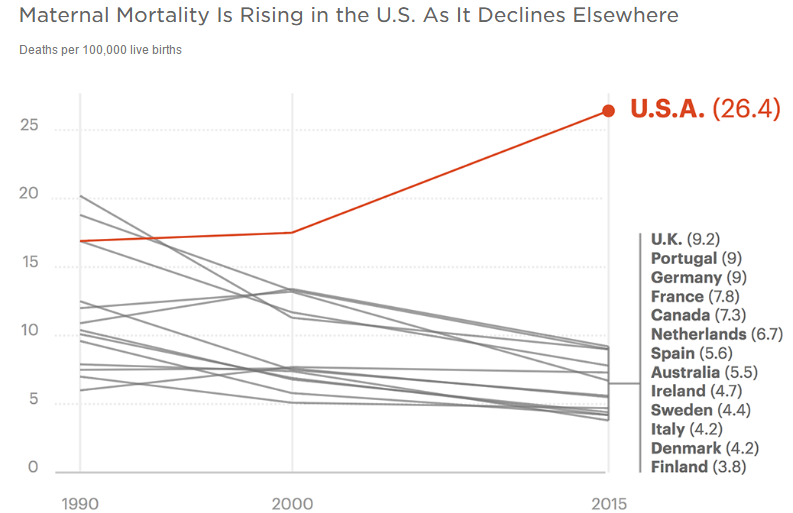




9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))


