A pair of refugees from Ukraine have resettled in Juneau.
Mayor Beth Weldon introduced Iryna and Ivan Hyrnchenko during a Juneau Assembly meeting on Monday. Weldon said they are the first Ukrainians to arrive in Juneau through a program that supports regular Americans who volunteer to help resettle refugees.
Iryna Hyrnchenko thanked Juneau for the warm welcome and spoke about the war in Ukraine.
“What is happening now in my country cannot be put into words,” she said. “There, we have our family and our hearts are with them. … I hope we found our new home here and life without fear. Thank you for all of your support and understanding.”
The Assembly gave them a pool pass and bus pass as welcome gifts.
The bulk carrier M/V Razoni leaves Ukraine’s port of Odesa on Monday. (Photo by Oleksandr Gimanov/AFP via Getty Images)
ODESA, Ukraine – A cargo ship loaded with 26,000 tons of Ukrainian corn left the country’s largest port Monday for the first time since Russia’s invasion on Feb. 24.
The milestone comes after the United Nations and Turkey signed agreements with Russia and Ukraine on July 22 to re-open Ukraine’s Black Sea ports and resume exports of grain, cooking oil and fertilizer. The U.N. had pushed for a deal to address a growing global food shortage.
Ukraine’s Infrastructure Minister Oleksandr Kubrakov filmed the ship, the Sierra Leone-flagged Razoni, as it departed and declared the U.N. deal “a great success for providing global food security.” He wrote on Facebook that Ukrainian ports would be working at full capacity in a few weeks.
Alla Stoyanova, Odesa’s agriculture chief, says Ukraine’s agricultural exports are even more important for its economy as a result of the war. (Photo by Joanna Kakissis/NPR)
Kremlin spokesperson Dmitry Peskov also noted the ship’s departure, calling it “very positive.” Russia signed a separate agreement with Turkey so it could export its grain and fertilizer, which remain grounded because of Western sanctions on banking and transportation.
The Ukrainians need this deal to work to keep their economy from falling apart.
“Ukraine used to earn 45 percent of its general income from the agriculture sector,” Alla Stoyanova, the Odesa region’s agriculture chief, told NPR. “Since the Russian invasion, practically every other sector has crumbled. So agricultural exports are now our money, our economy, our life.”
Russia’s war has cut off Ukrainian grain exports and exacerbated a global food crisis. (Photo by Joanna Kakissis/NPR)
Keeping up the pace of exports is crucial. Farmers continue to work during the war, sometimes donning helmets and bulletproof vests while working in their fields. They are running out of space to store crops. They can’t afford to plant next year’s crop.
Viacheslav Nevmerzhytskiy, who farms wheat and sunflowers near the port of Pivdennyi, not far from Odesa, says he worries that the Russians might even bomb the ships carrying Ukrainian products — and then try to pin it on Ukraine.
“I don’t see this shipping corridor lasting into the new year unless there are big security guarantees,” he says, like NATO guarding the ports.
Farmer Viacheslav Nevmerzhytskiy says he has doubts about how long the shipping corridor will last. (Photo by Joanna Kakissis/NPR)
Russia has repeatedly shelled the Odesa port and region since the grain export deals were signed. The Ukrainian military, meanwhile, is using specialists to remove undersea mines near the ship corridors.
Security is already tight at Ukrainian ports, which are now run by the military.
Dmytro Barinov, deputy head of Ukraine’s Seaport Authority, says at least 68 vessels have been stuck in the country’s Black Sea ports since the Russian invasion. About half are loaded with grain.
“Some of them continue to load,” he says. “They’re waiting (for) these corridors to work, and they can go out, perhaps in a kind of caravan on the sea.”
Hanna Palamarenko and Pavel Zilinskiy contributed reporting from Odesa.
Copyright 2022 NPR. To see more, visit https://www.npr.org.
Georgia Linders got sick with COVID in the spring of 2020 and never recovered. Her ongoing battle with long COVID has prevented her from working. She spends her days advocating for COVID longhaulers like herself and painting, one of the few activities that doesn’t wear her out. (Photo courtesy of Georgia Linders)
More than two years after Georgia Linders first got sick with COVID, her heart still races at random times.
She’s often exhausted. She can’t digest certain foods.
Most days, she runs a fever, and when her temperature gets up past a certain point, her brain feels like goo, she says.
These are commonly reported symptoms of long COVID.
Linders really noticed problems with her brain when she returned to work in the spring and summer of 2020. Her job required her to be on phone calls all day, coordinating with health clinics that service the military. It was a lot of multitasking, something she excelled at before COVID.
After COVID, the brain fog and fatigue slowed her down immensely. In the fall of 2020, she was put on probation. After 30 days, she thought her performance had improved. She’d certainly felt busy.
“But my supervisor brought up my productivity, which was like a quarter of what my coworkers were doing,” she says.
It was demoralizing. Her symptoms worsened. She was given another 90-day probation, but she decided to take medical leave. On June 2, 2021, Linders was terminated.
She filed a discrimination complaint with the government, but it was dismissed. She could have sued but wasn’t making enough money to hire a lawyer.
Survey data suggests millions of people aren’t working because of long COVID
As the number of people with post-COVID symptoms soars, researchers and the government are trying to get a handle on how big an impact long COVID is having on the U.S. workforce. It’s a pressing question, given the fragile state of the economy. For more than a year, employers have faced staffing problems, with jobs going unfilled month after month.
Now, millions of people may be sidelined from their jobs due to long COVID. Katie Bach, a senior fellow with the Brookings Institution, drew on survey data from the Census Bureau, the Federal Reserve Bank of Minneapolis and the Lancet to come up with what she says is a conservative estimate: 4 million full-time equivalent workers out of work because of long COVID.
“That is just a shocking number,” says Bach. “That’s 2.4% of the U.S. working population.”
Long COVID can be a disability under federal law
The Biden administration has already taken some steps to try to protect workers and keep them on the job, issuing guidance that makes clear that long COVID can be a disability and relevant laws would apply. Under the Americans with Disabilities Act, for example, employers must offer accommodations to workers with disabilities unless doing so presents an undue burden.
Linders now she thinks back to what she should have asked for after her return to work. She was already working from home due to the pandemic, but perhaps she could have been given a lighter workload. Maybe her supervisor could have held off on disciplinary action.
“Maybe I wouldn’t have gotten as sick as I got, because I wouldn’t have been pushing myself to do the things that I knew couldn’t do, but I kept trying and trying,” she says.
Dr. Monica Verduzco-Gutierrez, professor of rehabilitation medicine at the University of Texas Health Science Center at San Antonio, has seen COVID play out in similar ways in other patients.
“If someone has to go back 100% when they start feeling a little bit better, they are going to crash and burn fast,” she says.
Figuring out accommodations for long COVID can be complicated
The problem with coming up with accommodations for long COVID is that there are so many unknowns. The duration and severity of symptoms varies wildly from person to person.
Gutierrez finds herself stumped by questions on disability forms that ask how long an individual might be out or how long their illness may last.
“This is a new condition,” she says. “We don’t know.”
Accommodations in the workplace might include flexibility in where someone works, extended leave, or a new role in a different department. The goal is to get workers on a path back, says Roberta Etcheverry, CEO of Diversified Management Group, a disability management consulting firm.
But with long COVID, it’s difficult to measure whether an employee is in fact on a path back.
“This isn’t a sprain or strain where somebody turns an ankle and we know in x amount of months, they’re going to be at this point,” she says. “It’s not — somebody was helping move a patient, and they hurt their back, and they can’t do that kind of work anymore. They need to do something else.”
With long COVID, symptoms come and go, and new symptoms may arise.
The Labor Department is urging employers not to rule out accommodations for employees who don’t get an official long COVID diagnosis.
“Rather than determining whether an employee has a disability, your focus should be on the employee’s limitations and whether there are effective accommodations that would enable the employee to perform essential job functions,” the Labor Department says in its long COVID guide for employers.
Accommodations may be harder to come by in some jobs
Still, not all employers have the means to offer the kind of accommodation an employee may need given their symptoms.
Bilal Qizilbash believes he would have been fired long ago had he not been the boss of his own company.
“Majority of my team has no idea that I’m working from bed most of the time,” says Qizilbash, a COVID long hauler who suffers chronic pain that he compares to wasp stings.
As the CEO of a small business that manufactures health supplements, Qizilbash says he tries to be compassionate and at the same time, ruthlessly efficient. Having one employee whose productivity is severely compromised could end up negatively impacting the whole company, he says.
In other professions, it may be challenging to find accommodations that work, no matter how generous.
In South Florida, Karyn Bishof was a new recruit with the Palm Beach Gardens Fire Rescue team in 2020 when she contracted COVID, likely at a training, she says. She comes from a family of firefighters, and it was her lifelong dream to follow suit. She was excelling in her training and receiving high marks when she got sick, she says. Now long COVID has left her with profound brain fog, fatigue, light-headedness and a slew of other symptoms incompatible with fighting fires.
“I couldn’t run into a burning building if I can’t regulate my temperature,” she says. “If I can’t control having hypertension, I can’t lift up a patient or I’m going to pass out.”
The city of Palm Beach Gardens told NPR Bishof was terminated from her job for not meeting performance-related probationary standards. Bishof recently filed a discrimination lawsuit against the city and has become an advocate for COVID long haulers.
The Labor Department is crowdsourcing ideas for how to keep workers employed
Taryn Williams, Assistant Secretary of Labor for Disability Employment Policy, wants to hear from workers and employers. Through the middle of August, the Labor Department is holding an online dialogue, asking for input on policies that may help with workplace challenges arising from long COVID.
“We want to be responsive,” says Williams. “We’re considering how can we support these workers in what is a transformative time in their life.”
She says the government has encountered situations in the past when there was a sudden rise in the number of people needing accommodations at work. Significant numbers of service members returned from Iraq and Afghanistan with traumatic brain injuries, for example. Williams says such times have led to shifts in disability policy in the U.S.
From her home in La Crosse, Wisconsin, Linders has contributed a number of comments to the Labor Department’s online dialogue. Like Bishof, she also spends a lot of time helping other COVID long haulers navigate what she’s been through, including qualifying for Social Security disability insurance.
Her advocacy helps her feel as if she’s contributing something to society, even if it’s not the life she wanted.
“I don’t want to be disabled. I don’t want to be taking money from the government,” she says. “I’m only 45. I was going to at least work another 20 years.”
Copyright 2022 NPR. To see more, visit https://www.npr.org.
Transcript :
AYESHA RASCOE, HOST:
Close to 20 million adults in the U.S. are believed to have long COVID symptoms right now, according to the Census Bureau. And many of them are reporting that they can’t work through the brain fog, the chronic fatigue and pain that they’re suffering. NPR’s Andrea Hsu has talked with COVID long-haulers and with researchers about the impact long COVID is having on the American workforce. And she joins us now.
Welcome.
ANDREA HSU, BYLINE: Hi, Ayesha.
RASCOE: So the scale of this – it sounds really daunting. Do researchers know how many people have been sidelined from their jobs because of long COVID?
HSU: Well, several surveys have found that roughly a quarter of people with long COVID report that they can’t work, or they’re working less because their symptoms are so debilitating. I talked with Katie Bach. She’s a fellow with the Brookings Institution. She did some math and came up with what she says is a conservative estimate, 4 million full-time equivalent workers out of work due to long COVID.
KATIE BACH: That is just a shocking number. That’s 2.4% of the U.S. working population.
HSU: And then she went a step further to see, how much in wages do these people stand to lose if they’re not working?
BACH: Using just average wage, it’s about $230 billion a year in lost earnings.
HSU: Now, of course, some of these people may have paid leave, and others may still be getting a full paycheck, even if they’re working less than full time. But, Ayesha, all indications are that worker productivity is really suffering because of long COVID.
RASCOE: You spoke with people who have struggled to stay employed. Like, what are you hearing from them?
HSU: Well, some of the stories are really heartbreaking. I talked to Karyn Bishoff in Florida. She was a new recruit with the Palm Beach Gardens Fire Rescue team in 2020 when she got COVID. She believes she got COVID at one of her trainings. And now, more than two years later, she still has profound brain fog, fatigue, lightheadedness and a slew of other symptoms. And she realizes she will never be a firefighter.
KARYN BISHOFF: Like, I couldn’t run into a burning building if I can’t regulate my temperature. Like, if I can’t control having hypertension, I can’t lift up a patient, or I’m going to pass out.
HSU: So she hasn’t been able to work. She’s pretty much bedbound. But she has become an advocate. She’s created a support network online, and she’s pushing for policy changes. She’d like to see the Social Security Administration step up its processing of long COVID disability applications. But the problem here, Ayesha, is there’s so much variability. Even doctors are saying they have no clue how long it might take people to recover. And of course, not everyone is as ill as Karyn Bishoff. Other COVID long-haulers are able to work, although maybe more slowly or in shorter spurts. But still, it’s very concerning. And the Labor Department is trying to find ways to keep people employed.
RASCOE: So what can the Labor Department do?
HSU: Well, they’ve issued guidance stating clearly that long COVID can be a disability. And why that’s important is that people with disabilities have protections under the law. So, for example, employers are required to provide accommodations to workers with disabilities unless doing so presents an undue burden. Accommodations might be working from home or flexible hours. It could be extended leave or maybe a transfer to a different role. Now, of course, not every company can do that, but the Labor Department is urging employers to explore the possibilities. And they’re also holding what they call a virtual crowdsourcing event to gather ideas for what else could make a difference. I spoke with Taryn Williams. She heads up the Labor Department’s Disability Employment Policy Office.
TARYN WILLIAMS: We strongly encourage folks to take advantage of that online dialogue to help inform us on what we should be considering.
HSU: They want to hear from employees, employers, people with expertise in disability employment. You can Google long COVID at work idea scale – that’s S-C-A-L-E – to submit comments.
RASCOE: Has the American workforce ever faced, like, a situation like this before, having so many people at once suddenly needing accommodations for disabilities?
HSU: Well, I asked Taryn Williams that, and she pointed to times of war. Significant numbers of servicemembers did return from Iraq and Afghanistan with traumatic brain injuries, for example. And Williams said it’s been times like these that have led to shifts in disability policy. So we may see that happen now with long COVID, too.
RASCOE: NPR’s Andrea HSU, thank you so much.
HSU: You’re welcome. Transcript provided by NPR, Copyright NPR.
Dani Marietti’s “sterilization shower” in Helena, Montana, features cookies with abortion-rights slogans, such as “My Body, My Choice,” written on them in frosting. (Photo by Ellis Juhlin/Yellowstone Public Radio)
In July, a handful of people gathered in the shade of a large pine tree in Helena, Montana for a going-away party of sorts.
Their friend, Dani Marietti, was going to have her fallopian tubes removed.
It was a decision she had made after a draft of the U.S. Supreme Court’s decision to overturn the constitutional right to abortion was leaked to the press.
The small group kicked off the “sterilization shower” for the 25-year-old by laying out chalk-written signs that said “See Ya Later Ovulater” and “I got 99 problems but tubes ain’t one.” They munched on cookies that had abortion-rights slogans, such as “My Body, My Choice,” written on them in frosting.
Marietti is a full-time graduate student in Helena working toward becoming a therapist. She doesn’t want kids to get in the way of her career. She had considered permanent sterilization before, but the possibility that the Supreme Court would overturn Roe v. Wade pushed her to seek out an OB-GYN who would help her with a permanent method of contraception.
“‘I want to do this as soon as possible,'” she recalled telling the doctor.
“I always knew I didn’t want children, and of course when you say that as a younger person, everyone is like, ‘Oh, you’ll change your mind,’ or, ‘Just wait until you find the one,'” Marietti says. “I always kind of ignored that.”
Doctors see growing demand for sterilization
Abortion is still legal in Montana, but whether it will remain so is unclear.
State Attorney General Austin Knudsen, a Republican, has asked the Montana Supreme Court to overturn its 1999 decision that said the state constitution’s right to privacy includes the right to end a pregnancy.
The uncertainty around abortion access in Montana and other states where abortion is now or could become illegal, plus the fear of future legal fights over long-term contraception, has seemingly spurred a rise in the number of people seeking surgical sterilization, according to reports from doctors. That includes Marietti, who is having a salpingectomy — a procedure in which the fallopian tubes are removed instead of tied, as in tubal ligation, which can be reversible.
How many people sought permanent sterilization after the fall of Roe won’t become clear until next year, says Megan Kavanaugh, a researcher for the Guttmacher Institute, which gathers data related to reproductive health care across the U.S. and supports abortion rights.
But anecdotal reports indicate that more people have been undergoing permanent birth control procedures since the Supreme Court’s June 24 decision in Dobbs v. Jackson Women’s Health Organization, which struck down Roe.
Dr. Kavita Arora, who chairs the American College of Obstetricians and Gynecologists’ Committee on Ethics, says providers across the country are beginning to see an influx of patients into their operating rooms.
Arora, an OB-GYN in North Carolina, recounted what one of her patients said just before a recent surgery: “She wanted to have autonomous control over her body, and this was her way of ensuring she was the person who got to make the decisions.”
More adults in their 20s and 30s without children are coming to the hospital for sterilization consultations, says Dr. Marilee Simons, an OB-GYN at Bozeman Health Deaconess Hospital in Montana.
Many are women who already use long-term birth control options, but “they are still worried about an unintended pregnancy and what that might mean in the future,” she says.
Most are asking to have their tubes removed to permanently prevent pregnancy. A smaller number of people are asking for hysterectomies, which surgically remove part or all of the uterus. To meet demand, Bozeman Deaconess has dedicated at least one provider to work with these patients multiple days a week.
Planned Parenthood of Montana President and CEO Martha Fuller says clinics statewide have seen an “unprecedented” increase in patients asking to be sterilized, including requests for vasectomies.
Dani Marietti (holding sign) and her friends gather for a “sterilization shower” in Helena, Montana, in July before Marietti was scheduled to have her fallopian tubes surgically removed. (Photo by Ellis Juhlin/Yellowstone Public Radio)
Patients face obstacles
But some people seeking sterilization procedures across the U.S. are being turned away.
Arora says patients who don’t have children and are in their childbearing years are reporting difficulties finding physicians willing to sterilize them. Their reluctance may stem from studies that suggest patients who are sterilized at age 30 or younger are about twice as likely as those over 30 to express regret after getting the procedure. However, other studies had mixed results and found that some women feel less regret over time.
Some patients who have been denied sterilizations have turned to therapists like Barbara DeBree, who has a private practice in Helena and writes letters to providers attesting that the patients have thought through their decisions. “This is not a quick decision for them,” DeBree says.
Cost and insurance coverage can also be issues for patients seeking sterilization procedures.
Helena resident Alex Wright, 23, doesn’t plan to have children and wants to be sterilized.
She plans to schedule a consultation to see whether her provider will perform the procedure. If her regular provider won’t do it, she says she will seek out someone from online lists of providers who are willing to perform the procedure on younger people.
“That’s only helpful if I can get the financial assistance to get it taken care of through those people,” she says. Wright says her insurance company estimates she’ll pay about $4,000 out-of-pocket if she goes with an in-network provider. Using an out-of-network doctor could cost substantially more.
Some fear future “attacks on contraception”
Although some people are seeking permanent procedures in reaction to the Dobbs decision, others are doing so because they believe the U.S. Supreme Court will continue upending reproductive health norms.
Kavanaugh, the researcher at Guttmacher, says Justice Clarence Thomas opened that door by suggesting in his concurring opinion in Dobbs that other precedents should be revisited, including the 1965 Griswold v. Connecticut decision that says banning contraceptives violates a married couple’s right to privacy.
“I think we are anticipating that there’s going to be some attacks on contraception,” Kavanaugh says.
That’s what worries Shandel Buckalew, of Billings, Montana, who wants a full hysterectomy.
The 31-year-old says her doctor thinks she has endometriosis, a painful condition in which tissue that normally grows inside the uterus grows on other parts of the reproductive organs. Buckalew hasn’t undergone the full range of testing that can be required for a diagnosis because she doesn’t have health insurance and can’t afford it.
“Even though I have an IUD [intrauterine device], the amount of cramps and the pain I go through — oh, I get so sick,” she says.
Buckalew hopes a hysterectomy will alleviate that pain, in addition to providing permanent birth control because she doesn’t want kids. But her lack of health insurance makes the procedure unaffordable.
She’s trying to get health insurance before her IUD expires in two years, because she fears the reproductive health care landscape could shift dramatically.
“It feels like my life doesn’t matter,” she says.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Copyright 2022 Kaiser Health News. To see more, visit Kaiser Health News.
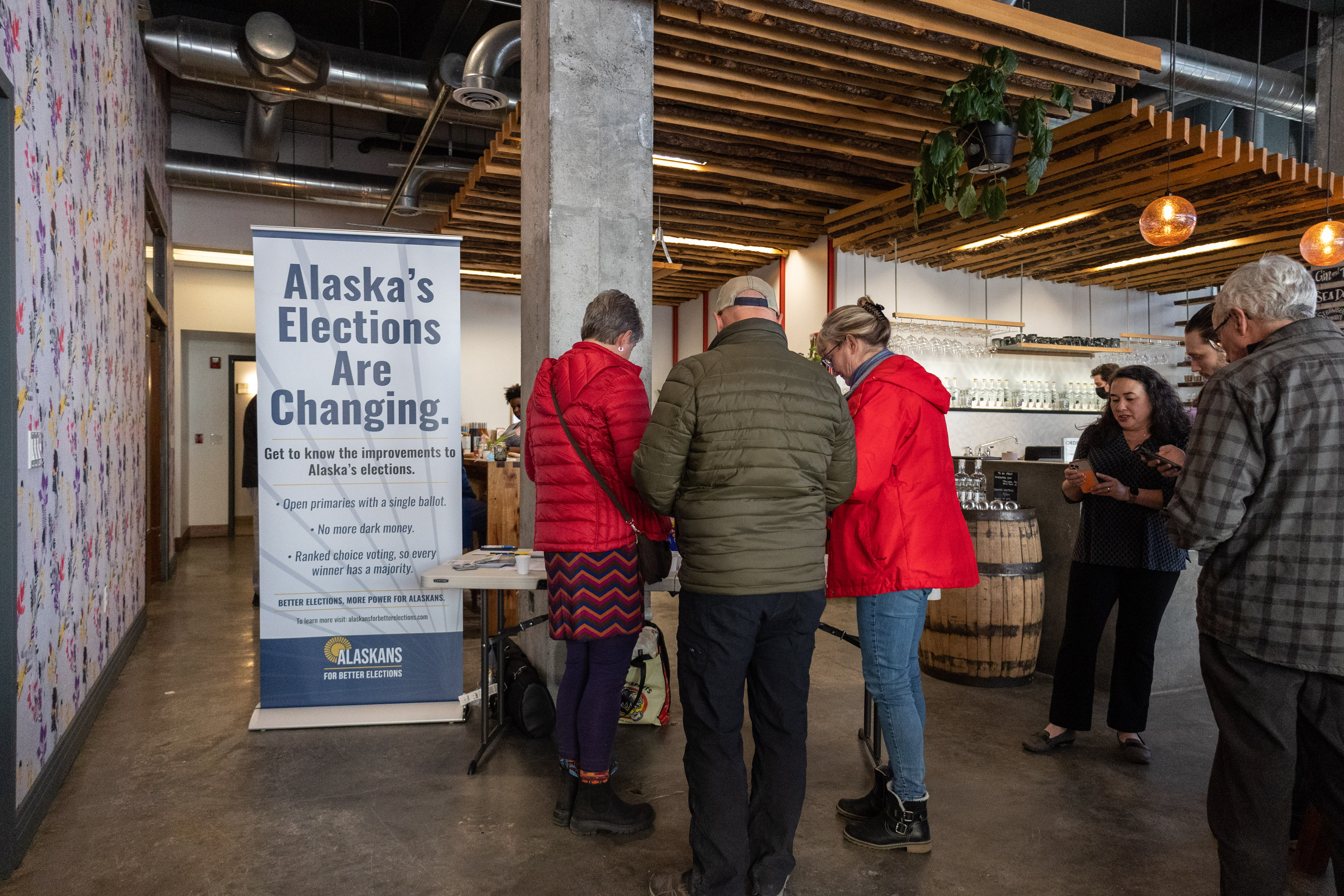
Alaskans For Better Elections hosts an event educating people about ranked choice voting at Amalga Distillery in Juneau, Alaska on April 19, 2022. (Photo by Lyndsey Brollini/KTOO)
The 2022 midterm elections are on the horizon. This will be Alaska’s first time using ranked choice voting for statewide races. Are you planning to vote? Do you know how to vote, where to vote, and what you might need to have when you show up to the polls? What if your voter registration is out of date or has a mistake, and you get challenged at the polls — what can you do?
KTOO is part of a new community-powered journalism project to answer those questions and any others you have about how to exercise your right to vote in the upcoming election. Our mission is to provide you with the information you need to vote.
We’re not concerned about how you vote and especially not about who you vote for. We just want to make sure you are armed with the information you need to vote and understand how elections are run and kept secure.
This project is part of the work of America Amplified, an initiative funded by the Corporation for Public Broadcasting to support community engagement journalism in public media. We’re also working with 28 other public media stations across the country to ensure that all eligible American citizens can vote.
Many states, including Alaska, have changed voting regulations since the 2020 general election when concerns about the pandemic led to an expansion of absentee and mail-in voting. This time around the rules are different, and there’s a ton of misinformation and disinformation circulating about elections and election security. We’re here to clear things up.
You can’t change anything unless you choose to participate in the process. We’re asking you to participate by sending us any and all questions about taking part in the upcoming election.
With help from our partners at America Amplified, we’ll answer the questions online, on the air and on social media. We’ll send the answers directly to you as well. If you share your contact information, we may even reach out personally. We can’t do this without you. Gunalchéesh!
The FDA is trying to make “bivalent” COVID vaccines, which target two different antigens, available as soon as September. (Photo by Robyn Beck/AFP via Getty Images)
The Biden administration may scrap plans to let more younger adults get second COVID-19 boosters this summer. Instead, officials are trying to speed up availability of the next generation of boosters in the fall, NPR has learned.
The new strategy is aimed at trying to balance protecting people this summer with keeping people safe next winter, when the country will probably get hit by yet another surge.
But the possible shift is being met with mixed reactions. The Food and Drug Administration could make a final decision by the end of the week.
The dilemma facing the FDA is that the immunity many people have gotten from getting vaccinated or infected has been wearing off. At the same time, the most contagious version of the virus to emerge yet — the omicron subvariant BA.5 — is making people even more vulnerable.
But letting more people get boosted with the original vaccine now could interfere with plans to boost them with updated, hopefully more protective vaccines in the fall to blunt the toll of the winter surge.
That’s why the administration is considering shifting the focus to the next generation of boosters. Moderna and Pfizer-BioNTech were already scrambling to comply with the FDA’s request to get new, hopefully more powerful “bivalent” boosters ready by October or November that target both the original strain of the virus and omicron subvariants BA.4 and BA.5.
The FDA is trying to get the companies to make those shots available even sooner — possibly as soon as September, according to a federal official familiar with the situation who is not authorized to talk about it publicly. The possible shift was first reported by The Washington Post.
If the bivalent boosters can be accelerated, the FDA would skip opening up fourth shots of the original vaccines this summer and just wait for the new double-barreled omicron vaccines in the fall.
The possible shift is provoking mixed reactions.
Some think it is the smartest strategy. Three shots are still protecting most younger, otherwise healthy people against serious illness, they say. And boosting people again now, and then so soon again in the fall, could confuse people, potentially eroding their willingness to get any boosters, according to some experts.
“I think this will increase trust,” Dr. Monica Gandhi, a professor of medicine at the University of California, San Francisco, wrote in an email to NPR. “We can’t give a booster now and then again in 1.5 months or two months – that will decrease trust.”
And giving two shots too close together could actually backfire from a health perspective, according to some experts.
“I think this is the right call,” Dr. Celine Gounder, a senior fellow at the Kaiser Family Foundation, said during an interview with NPR. “If you get a booster now with the original formulation of the vaccine, this may in fact be counter-productive. It may prevent the second booster dose given this fall from taking and from you developing an immune response to that booster.”
But others aren’t so sure. They say the new vaccines may not be significantly better.
“People should not regard them as some sort of magic bullet that gives them super-strong protection,” says Dr. John Moore, an immunologist at Weill Cornell Medicine. “These are not going to be magic bullet game-changers because they’re not that much better than the already available vaccine boosters.”
It’s also unclear whether the new boosters can be ready by September. And who knows if BA.5 will even been the main virus by the fall and winter?
“I don’t see the benefit waiting for a BA.5-specific booster since BA.5 may be in the rearview mirror and well past us by the time that’s available,” says Dr. Peter Hotez, dean of the Baylor College of Medicine National School of Tropical Medicine.
People younger than 50 should at least have the option to protect themselves now, especially with BA.5 already surging, some say.
“You’re talking about you know literally hundreds of millions of people who are at a higher risk than they need to be for months,” says Dr. Robert Wachter, chair of the department of medicine at the University of California, San Francisco.
“And that will mean potentially millions of preventable infections, certainly thousands of preventable hospitalizations, and probably hundreds of preventable deaths.”
Copyright 2022 NPR. To see more, visit https://www.npr.org.
Close
Update notification options
Subscribe to notifications
Subscribe
Get notifications about news related to the topics you care about. You can unsubscribe anytime.






9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))

9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))


9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))
9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))