The Legislature completed the first stage of its annual budget process today. House Finance Subcommittees recommended more than $120 million more in cuts on top of the $100 million that Gov. Bill Walker proposed.
Health and Social Services was the department that received the deepest cuts. They include eliminating $5.18 million in cash assistance to seniors, and $3 million in behavioral health grants.
Rep. David Guttenberg, a Fairbanks Democrat, opposed the cuts. He said reducing treatment of people with addictions will cost the state more in the long run.
“These grants will clearly prevent increases in costs in other places, in the courts, in the Department of Law, in our prisons, in our various higher-end costs,” Guttenberg said. “Dealing with folks that have issues and troubles at the most efficient place to touch them, is something that we need to do.”
Overall recommended cuts to Health and Social Services total $41 million, roughly one-third of all cuts that finance subcommittees recommend.
Rep. Dan Saddler, an Eagle River Republican, compared the difficulties faced by those with addictions to the choices the Legislature faces.
“There are many unfortunate and difficult challenges we face in life and running away from them in a bottle or a needle is not the way to solve them,” Saddler said.
“The way to get through problems is to face the difficult choices and to make difficult choices. And I think that is what we’re doing in this budget, and that’s what we’re doing in this particular allocation. In addition to a heroin crisis in Alaska, we have a fiscal crisis in Alaska. And I think we are making the difficult, but responsible decisions to scale our resources to meet our needs the best way we can.”
Health Commissioner Valerie Davidson during a discussion on Medicaid reform in Senate Finance Feb. 24, 2016. (Photo by Skip Gray/360 North)
Health and Social Services Commissioner Valerie Davidson said she’ll be working to inform legislators about the exact effects of the proposed cuts before the entire Legislature finishes its work on the budget this spring.
“We’ll definitely continue to work with members of the Legislature,” she said. “We realize that cuts have to be made. And our job is to make sure that everybody understands the implications of the cuts that are being made.”
Institute of Social and Economic Research economist Gunnar Knapp said that budget cuts will have broader impacts on Alaska’s economy, along with the direct effect on services.
Institute of Social and Economic Research Director Gunnar Knapp presents possible economic effects of state budget proposals to the Houses Finance Committee, Feb. 25, 2016. (Photo by Skip Gray/360 North)
Knapp told the budget committee on Thursday that for every $100 million in broad-based cuts to state government, the state will lose 1,260 jobs and $115 million in income.
In comparison, introducing a similar amount in income taxes would impact fewer jobs, but could mean 20 percent more lost income.
Knapp urged legislators to close the state’s $3.5 billion dollar budget shortfall.
“The smoothest transition is to make a significant start on reducing the deficit this year,” Knapp said. “Not making major progress this year would have a big impact. The rating companies have promised that they would further downgrade our credit ratings and then there would be impacts due to a loss of business confidence and reduced private investment.”
The Legislature will hear public testimony on the budget next week (Feb. 29 to March 3) at locations across the state.
Rachel Star Withers says that video blogging about schizophrenia and depression has helped her manage the disorders. Courtesy of Rachel Star
When she was 22, Rachel Star Withers uploaded a video to YouTube called “Normal: Living With Schizophrenia.” It starts with her striding across her family’s property in Fort Mill, S.C. She looks across the rolling grounds, unsmiling. Her eyes are narrow and grim.
She sits down in front of a deserted white cottage and starts sharing. “I see monsters. I see myself chopped up and bloody a lot. Sometimes I’ll be walking, and the whole room will just tilt. Like this,” she grasps the camera and jerks the frame crooked. She surfaces a fleeting grin. “Try and imagine walking.”
She becomes serious again. “I’m making this because I don’t want you to feel alone whether you’re struggling with any kind of mental illness or just struggling.”
At the time, 2008, there were very few people who had done anything like this online. “As I got diagnosed [with schizophrenia], I started researching everything. The only stuff I could find was like every horror movie,” she says. “I felt so alone for years.”
She decided that schizophrenia was really not that scary. “I want people to find me and see a real person.” Over the past eight years, she has made 53 videos documenting her journey with schizophrenia and depression and her therapy. And she is not the only one. There are hundreds of videos online of people publicly sharing their experiences with mental illness.
In her early videos, Withers glowers. She tried to give off an aura of toughness befitting the daughter of a Hell’s Angel biker. But there’s also a sense that terror is a deep undercurrent in her life. “All right, let’s go,” she says in the video “Watch If You Forget,” where she documents getting electroconvulsive therapy for depression. Then, in the next few seconds, “I’m about to start the electroshock therapy and, yeah, I’m pretty nervous.”
Things have changed a lot since then. Now, almost all her videos open with Withers flicking her black curls, arms raised with swagger: “Hey, what’s up! I’m Rachel Star!”
That public sharing of mental illness might be making a huge impact on the way our society views these disorders, especially for those of us who are digital natives. Millennials tend to be more comfortable talking about mental health issues, according to a poll released Jan. 14 by the Anxiety and Depression Association of America, along with two national suicide prevention foundations.
When it came to seeing a mental health professional, for instance, 48 percent of survey respondents between the ages of 18 and 34 said that it was a sign of strength. About 35 percent of all prior generations felt the same way.
“Our young people are accepting that mental health problems exist, and they want help for it, and they are not looking at these things as something to be ashamed of,” says Anne Marie Albano, a clinical psychologist at Columbia University who is on the board for the ADAA.
She thinks that social media and videos like Withers’ have helped lower stigma around mental illnesses. “Young people take advantage of this,” Albano says. “It gives the opportunity for people to tell their stories and post images. This allows them to feel more hope than prior generations.”
There might be other reasons young people are less concerned about stigma surrounding mental illness. Perhaps as you age, your outlook becomes more pessimistic, says John Naslund, a Ph.D. candidate at the Dartmouth Institute for Health Policy and Clinical Practice who studies social media and mental health. He notes that the ADAA poll found that a higher percentage of older adults than young people didn’t believe that something like suicide could be prevented. “Maybe they’ve been through this before and have had people close to them take their own lives.”
He hopes things really are getting better. “It’s very possible. That would be a very exciting change in the way society views mental illness,” Naslund says. But the problem has not been solved. Even if information moves quickly, change is slow. “It’s really important to acknowledge that people who have serious mental disorder still face a lot of stigma,” he says.
When she was younger, Withers struggled with a lot of shame and humiliation over her disorders. “For so many years, I felt like a freak,” she says. Part of that was the religious community she had joined. “Think militant Christian. Like a militaristic type,” she says. When she was 17, she graduated from high school early to attend the former Teen Mania Ministries Honor Academy in Dallas. “I honestly thought that’s what God wanted me to do.”
At the same time, her mental condition was deteriorating. She says her schizophrenia was starting to emerge and transform into something unmanageable. The counselor at Honor Academy diagnosed her with depression and prescribed pills. They didn’t help. Eventually she told them about her hallucinations. “This being a Christian place, they decided I was possessed by demons.”
For three days, Withers fasted. Each morning, she met three of the school’s spiritual advisers, and they spent the day performing an exorcism in a closed room. They read Bible verses, and Withers confessed to everything she could think of that might be construed as a sin — even watching demon-related TV shows like Buffy The Vampire Slayer.
At the end of the crucible, Withers was on the floor, exhausted. “I was young and here are these people who you know, I’m told, are close to God. I was like … OK. It must be right,” she says. “Surprise! It didn’t work. I spent six more months there as an outcast.”
Reducing this kind of stigma is a fundamental reason Withers continues making videos. She wants others to see those struggling with mental disorders with more compassion, and she wants people with a mental diagnosis to see themselves more positively.
YouTube
After she posted her first video, Withers says, “People just come out of the woodwork emailing me, messaging me. The friends I’ve had the longest time, even people I’ve never met in real life with schizophrenia and like disorders. We just started talking.” She got invited to mental health forums and to mental health support groups on Facebook.
“Thank you for these videos. They really help me to better understand my sister,” YouTube user Kathryn Hatzenbuhler posted under one video.
These online communities are an important part of Withers’ life now. “Whenever I’m posting on Twitter, I’ll put #schizophrenia and #schizophrenic. I’m hoping to find other people who are having problems,” she says.
Withers ended up making a coloring book for kids with schizophrenia, and she shares ways she has figured out to deal with her visions and voices.
Via webcam, she showed me two askew mirrors in her room that can be angled away from the viewer. “People with mental disorders don’t do well with mirrors. I just start hallucinating,” she says. “It’s real hard putting on makeup, you have to imagine. Having the mirrors at an angle helps.”
In one video, she talks about walking up to one of her hallucinations to touch it, and that alone took away some of the fear. “It’s kind of something to help you get used to your hallucinations, so you know how to respond, because the voices are always horrible. The voices are never like, ‘Oh my God, you look so good today.'”
There’s no hiding her disorder from anybody on Facebook, so people she knew in real life started finding out. It caused her pain at some jobs (“This one girl was like, ‘Oh she’s crazy. I’m not working with her’ “), but it also led some people to talk about their own or their family’s experiences with mental disorder. “They’ll be like, ‘So … I saw your post, Rachel. I had a question.’ ”
Researchers think there’s a potential gold mine of mental health benefits in exchanging messages and encouragement online like this. “Social support is always the No. 1 variable that predicts a better prognosis and better care management of anyone’s illness,” Albano says.
It’s a small leap from there to think that participating in mental health-focused communities on YouTube and Facebook might actually be making people healthier and preventing suicides. “That’s probably absolutely correct,” says Patrick Corrigan, a professor of psychology at the Illinois Institute of Technology. But scientists are only just now beginning to measure the effect social media might have on clinical outcomes. “It’s quite a new area of thinking, online peer-to-peer support for mental illness,” Naslund says.
But there’s an obvious downside to being public on social media about mental health problems. “Say I have a network of friends and I have a breakdown one day. It will spread through social media, maybe in negative ways,” says Michael Lindsey, a professor of social work at New York University. That could be through someone’s real social groups, like at work or school, or it could be anonymous, via Internet trolls. For those already depressed, anxious or paranoid, cruel comments and messages could have a terrible impact.
But in Naslund’s research, he says that problems with online attacks have been extraordinarily rare. “If someone did post a derogatory comment, seemed a little harmful, other people would come to the defense and say, ‘Don’t listen to that,’ ” he says. “[Social media are] way more supportive than we imagined.”
According to Naslund, the benefits seem to vastly outweigh the harms. “That’s clear in the literature,” he says.
And Withers agrees. She doesn’t think that people with mental health problems usually go on social media and spiral out of control even more. “I’m sure it happens somewhere on some area of the Internet,” she says. “But I think usually when I’m feeling depressed and stuff, but then I see someone else thinking of hurting themselves, the opposite kicks in. It’s like, no. You have so much to live for. You’re able to pull yourself out in a way to help someone else.”
When Withers does get trolls, she blocks them. “Anything remotely violent towards me gets blocked,” she says. “Like — I’m not going to respond to that. Don’t call me that word.”
Still, she cautions others to think carefully before coming out to the world about their mental illness. It can be dangerous, she admits. She says she gets phone stalkers and death threats. But she is still glad that she did it. It’s uncomfortable for her to think what might have happened if she never went online about her depression and schizophrenia. “I see myself being a lot more closed off,” she says. “I hope I would have found other people’s videos.”
Withers attributes a lot of her transformation to electroconvulsive therapy. She says it knocked out a lot of her deep depression. And Withers thinks sharing on the Internet has also helped. “It helps me to vocalize it and put it all out there,” she says, and it makes her feel like she is less “broken and sick” when other users empathize with her online.
Recently, she posted a video to YouTube called “There Will Be Beautiful Days.” It’s short, reaching just past a minute long. Withers smiles and says she knows things are hard now. Maybe harder than they’ve ever been. But it’s going to be OK. And at some point, you’ll have some good days. Maybe even just one great day, but it’ll be enough. It will make life worth fighting for.
Copyright 2016 NPR. To see more, visit http://www.npr.org/.
Read original article – January 27, 2016 2:05 PM ET
Cheryl Woolnough, director of training at Patriot PAWS in Rockwall, Texas, works with Papi, a Labrador retriever. Lauren Silverman/KERA News
At a warehouse near Dallas, a black Lab named Papi tugs on a rope to open a fridge and passes his trainer a plastic water bottle with his mouth.
Service dogs are often trained to help veterans with physical disabilities. Now, a growing number are being trained to meet the demand from vets with post-traumatic stress disorder and other mental health issues.
Those dogs learn extra tricks — how to sweep a house for intruders, for example, so a veteran feels safe.
“We teach them something called perimeter, where they go into the house and they check, they just touch all the doors and all the windows,” says Cheryl Woolnough, training director at Patriot PAWS, a nonprofit in Rockwall, Texas, that provides service dogs.
These dogs also learn how to create personal space for a veteran by stepping in front or behind the owner to block people from approaching.
Most veterans who apply for a service dog have PTSD, often on top of physical disabilities, according to Terri Stringer, assistant executive director of Patriot PAWS. “We have 100 veterans on our list waiting for dogs, so we have to get more dogs,” Stringer says.
So far, though, the Department of Veterans Affairs won’t help pay for service dogs for PTSD, citing a lack of scientific evidence. But it’s launching a study to find out what effect specially trained service dogs can have on the lives of veterans with PTSD. Vets with PTSD who already rely on service dogs say the research should have been done years ago.
The training process for these service dogs is complex.
It starts with puppies — often Labs, poodles or Labradoodles. The little guys get their shots and learn simple commands first. Then they go either to a puppy raiser who teaches them to behave in public places or they go to prison, literally. Stringer calls it the “big doghouse.”
Jay Springstead, a Vietnam veteran who has post-traumatic stress disorder, started working at Patriot PAWS after his youngest son, an Iraq combat vet who also had PTSD, took his own life. Lauren Silverman/KERA News
“Prison is where they get their hard-core training,” she says. “They’re with the inmates 24 hours a day.”
The inmates teach the dogs dozens of commands. Patriot PAWS relies on three Texas prisons for the type of intensive training the dogs need to be paired with veterans. It takes more than two years and costs about $30,000 per dog. The few veterans lucky enough to make it to the top of the list each year get dogs at no charge.
Jay Springstead, who lives outside Dallas, still has nightmares from combat in Vietnam 40 years ago. “A service dog for post-traumatic stress can actually help you get out into the public and regain some of that independence that you’ve lost,” he says.
Springstead started volunteering at Patriot PAWS after his youngest son took his own life.
“Both my sons were Iraqi combat veterans; my youngest one had severe post-traumatic stress,” he says. “So I’m familiar with the symptoms and I also know how important dogs are to anyone’s recovery.”
Springstead and many others are frustrated that the VA is not providing financial assistance to veterans who use service dogs to cope with PTSD.
It’s a complaint Patricia Dorn, director of the VA’s Rehabilitation Research and Development Service in Washington, D.C., has heard repeatedly. She says that while there is plenty of scientific evidence of the benefits of service dogs for people with physical disabilities, there’s little in the area of mental health.
“We understand, veterans are not happy with the agency in that we’re not just providing this benefit,” Dorn says. “But for an agency with [over] 150 hospitals and millions of veterans we serve, we need to have the evidence base to make a determination.”
That’s why the VA is conducting a randomized controlled trial on service dogs with 200 veterans with PTSD from Atlanta; Iowa City, Iowa; and Portland, Ore.
Dorn says researchers will assess veterans’ quality of life over a three-year period.
This isn’t the first time the VA has tried to study service dogs and PTSD. An earlier effort was halted in 2011 after two service dogs bit children in veterans’ homes. The current study, Dorn says, has stricter standards for dog training and a more rigorous study design.
In the meantime, Springstead says veterans sometimes get tricked into buying dogs that aren’t properly trained. Patriot PAWS is one of a few dozen organizations in the country accredited through Assistance Dogs International, but there’s no standardized training specific to mental health.
Copyright 2016 KERA Unlimited. To see more, visit KERA Unlimited.
Read Original Article – Published January 4, 2016 4:19 PM ET
Homeless veteran James Thomas talks with officials in Miami. Miami-Dade County is one of hundreds of municipalities that had sought to end veteran homelessness by the end of this month. AP
The smell of coffee filled the air on a recent Thursday morning in Carpenter’s Shelter, a homeless shelter here, as about a dozen people milled about.
Two U.S. Army veterans were among them: a middle-aged man and woman who aren’t looking for a permanent place to live. They said the food, showers and services at the shelter are enough, for now.
The Obama administration, in June 2014, challenged local governments to find a home for all veterans who want one by the end of this month. At least nine states and 850 municipalities tried to meet the goal, but Virginia and 15 municipalities were the only ones that succeeded.
But even there, hundreds of veterans remain homeless, most often because they have mental health or substance abuse problems, or just want to live on the street. In Virginia, the two at Carpenter’s Shelter are among about 600 homeless veterans. There are hundreds more in the municipalities that met the goal — in Alabama, Florida, Illinois, Louisiana, North Carolina, Nevada, New Mexico, New York, Pennsylvania and Texas.
The goal did not require municipalities to show that all veterans had been housed — just to prove they could quickly provide shelter, if needed. And even in places that did find a home for most veterans, some of them found themselves on the street again.
Challenges
The fact that so few cities, and just one state, have met the challenge points to just how complex the issue is.
At Carpenter’s Shelter, staff comes at it with “a heavy dose of optimism, with some pragmatism, as well,” said Shannon Steene, the shelter’s director.
“They didn’t get here overnight,” he said, “and they probably aren’t going to get out of it overnight.”
In many of the states that still have thousands of homeless veterans on the streets — the largest populations are in California, Florida, New York and Texas — the biggest challenge is there simply isn’t enough affordable and suitable housing, people who work with homeless populations say. That’s a problem not just for the homeless, but for many middle-class families, and it’s one homeless advocates cannot solve on their own.
In San Diego, California, for instance, at least 200 veterans who have housing vouchers that would pay some of their rent aren’t able to find apartments because the vacancy rate is so low, said Phil Landis, president and CEO of Veterans Village of San Diego. The nonprofit has been helping homeless veterans since the 1980s.
“The greatest hurdle here isn’t the outreach and the motivation, it’s in finding suitable housing,” Landis said.
Success Stories
Cities large and small met the federal milestone this year. Philadelphia, with a population of about 1.6 million, announced Friday that it met the goal. Troy, New York, a city of about 50,000, met the goal in September.
Virginia, the first and only state to reach the goal, and New Orleans, the first city to do it, used similar tactics to attack the problem. They employed a “housing first” strategy of getting veterans off the streets, out of shelters, and into stable housing as the first step in trying to bring stability to their lives.
Local governments joined with advocacy groups to enlist a swarm of volunteers who walked the streets and visited shelters, handing out fliers and encouraging veterans to take advantage of the programs.
They made lists of the names of each veteran living on the street or in a shelter, and tried to help them one by one. And they checked back often.
Organizers convinced landlords to house the veterans, and gave the veterans vouchers to use to pay rent for as long as they need. Some nonprofits even signed their leases for them.
That’s known as “master leasing,” and Pamela Michell, director of New Hope Housing, an Alexandria nonprofit that uses the approach, said it provides residents and landlords with a go-between, should any problems arise.
The work is ongoing. Shelter workers continue to try to build relationships with veterans who still don’t have a roof over their heads, urging them to get off the streets and to get help with the problems that keep them from being permanently housed.
“I try to encourage them,” said Sharon Addison, coordinator of the day program at Carpenter’s Shelter in Alexandria. “I say, ‘The new year is coming up. The shelter’s next door, whose gonna go next year?’ Sometimes they go, sometimes they don’t.”
Addison gave both of the veterans who were in the shelter on that Thursday morning information about services weeks ago.
One of them, Aaron McCullough, 55, stays at the shelter some nights despite the fact he is paying $90 a week to rent a small room in a house in Fairfax, Virginia, a 20-minute bus ride away.
The shelter is closer to where he works. He said he would try to find a more permanent place, but he “doesn’t think it will work. It’s too complicated, or something. I’m saving money.”
The federal push to house homeless veterans also encourages the housing first approach of first providing shelter, before the underlying reasons for their homelessness — such as mental illness or drug addiction — can be addressed. Seventy percent of homeless veterans have substance abuse problems and half have a serious mental illness, according to the National Coalition for Homeless Veterans.
Virginia and Louisiana had both signed on to this strategy before the national effort to focus on homeless veterans. The model has often demonstrated that people are more likely to succeed when given a stable place to call home, according to a joint study by the U.S. Department of Veterans Affairs and the National Center on Homelessness Among Veterans.
Much of New Orleans’ progress was a result of the rapid re-housing system it put in place after Hurricane Katrina, in 2005, said Martha Kegel, director of Unity of Greater New Orleans, the nonprofit that has led homelessness efforts in the city since then. Rapid re-housing, like housing first, focuses on quick housing as the first step of intervention, but it focuses on homeless people with moderate needs only, not the chronically homeless.
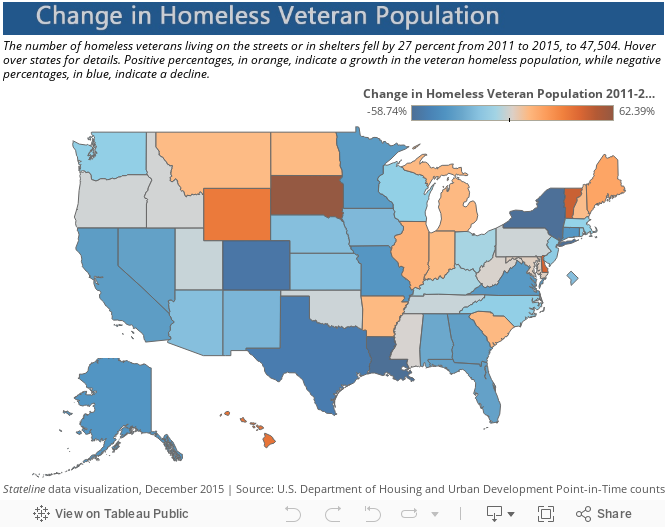
What New Orleans did became a model for other municipalities across the state, and it was largely successful. In Louisiana, the number of homeless veterans fell more than in any other state from 2011 to 2015, by 58.7 percent, to 392.
In Virginia, the number fell by 35.1 percent, to 604.
National Progress
This kind of progress has been seen nationwide. The number of homeless veterans living on the streets or in shelters fell by 27 percent, to 47,504, according to the annual count by the U.S. Department of Housing and Urban Development released last month.
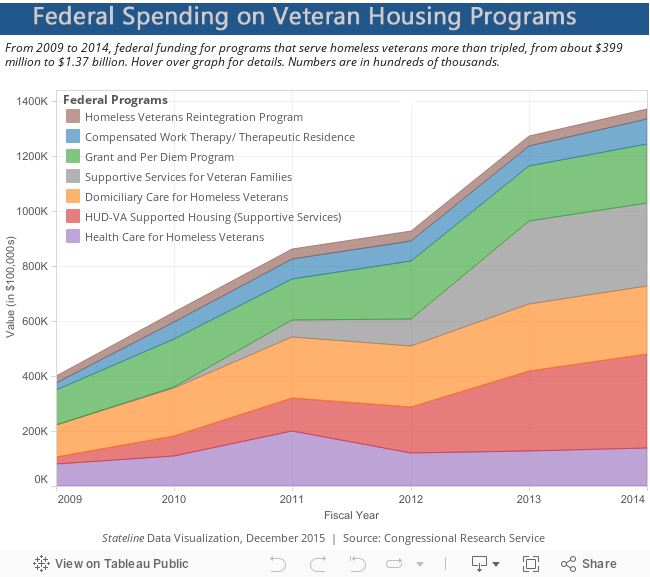
Colorado, Louisiana, New York and Texas made the most headway, all cutting their numbers by more than half. Even in California, where the average cost of monthly rent is 50 percent higher than in the rest of the country, the number of homeless veterans fell by 32.6 percent, to 11,311. Local groups say the decline came as federal funding funneled into their communities. In 2009, the VA made ending veteran homelessness a priority, and in 2014, the VA joined with HUD on new initiatives: the Mayors Challenge to End Veteran Homelessness and the 25 Cities Effort. Federal funding for programs that serve the population more than tripled from fiscal 2009 to 2014, from about $399 million to $1.37 billion, according to the 2015 Congressional Research Service. That included new veteran housing vouchers each year from fiscal 2009 to 2014, totaling $425 million. Appropriations for government-contracted nonprofits that work on housing for veterans totaled about $764 million nationwide from fiscal 2011 to 2014.
States and municipalities that have met the federal goal have proven that they have identified and reached out to all homeless veterans, and have the resources and systems in place to house any homeless veteran who wants to be housed, said Beverley Ebersold, regional coordinator at the U.S. Interagency Council on Homelessness.
The times veterans do face homelessness should be “rare, brief and nonrecurring,” Ebersold said.
Housing First Has its Critics
Housing first, the chief tactic used in the national battle, isn’t without its critics.
Landis, of Veterans Village of San Diego, said that while rapid re-housing is effective overall, it sometimes leaves veterans without the case management and mental health services they need.
His group runs a Veterans Treatment Center for those with substance abuse and mental health issues that provides case management and individual counseling. The organization receives about $2.4 million from the VA for the program, which funds 165 beds in the center. Those beds are always full, Landis said. But with the focus on housing first, he has heard that the money will soon dry up.
He and others in the city were upset to see the number of homeless veterans in San Diego rise from 2014 to 2015, from 1,307 to 1,381, despite their focused effort and increased funding.
He suspects the increase may be due, in part, to people who have been rapidly re-housed, without receiving the services they need to succeed.
“We don’t disagree that housing first has enormous positive impact,” Landis said. “But for those vets seeking treatment there should be at least one place in America where they can get it.”
Prince George’s County District Court in Maryland has used a mental health court as an alternative to traditional criminal proceedings. Sallicio/Wikimedia
Mental health courts have been embraced in many communities, and it’s easy to understand why.
Rather than sending someone who’s mentally ill to an overcrowded jail that is poorly equipped to manage his condition, mental health courts offer treatment and help with housing and other social services.
The community saves on the cost of locking someone up and offenders get support to stay healthy and may have their charges expunged.
Everybody wins, right?
The reality is more complex. Mental health courts have been in existence since the 1990s, modeled after drug courts that offer an alternative for people with substance abuse problems who are charged with drug-related crimes.
After initially accepting only those charged with misdemeanor crimes such as vandalism or trespassing, many of the roughly 350 mental health courts nationwide now accept people charged with some felonies such as robbery, and even violent crimes in some cases.
The approaches vary widely, but judges often oversee a team of mental health experts and social services case managers who refer participants to services available in the community. Offenders generally return to the court regularly for the judge to review their progress and offer encouragement or, if necessary, sanctions.
Research is still scant on the courts’ effectiveness at addressing offenders’ mental health problems or discouraging offenders from relapsing into criminal behavior. And some experts are concerned that offenders who are charged with minor crimes would be better off staying out of the criminal justice system and instead just getting treatment.
The popularity of mental health courts also aligns with growing concerns about prison crowding and the increasing costs to taxpayers. Estimates vary, but according to one study up to two-thirds of people in jails and prisons had a mental health problem in the previous year, compared with 11 percent of the general population.
In Florida, Judge Steve Leifman presides in the 11th Judicial Circuit for Miami- Dade County and oversees the mental health court. The approach there to dealing with mentally ill offenders is multilayered, Leifman says. Many arrests are averted by a crisis intervention team of police who refer people to treatment before they’re booked.
Offenders who are arrested and complete the mental health court program have a much lower recidivism rate than their peers: 20 percent versus 72 percent. “The key is to identify people and get them treatment earlier,” Leifman says.
A report by the Urban Institute that summarized research on mental health courts concluded that they seemed to be modestly effective at reducing recidivism, but it was unclear whether they had a positive effect on participants’ mental health.
These courts handle only a tiny fraction of cases dealing with mentally ill offenders, by some estimates 5 percent or less. Given their limited resources, it’s critical that mental health courts target the right people, generally those who are at highest risk for committing a new crime and who have serious mental illness, say experts.
From that perspective, the shift toward including people who are charged with more serious crimes and may be facing a sentence of several years makes sense.
“That’s when you start to see real cost benefits [to the system] in that you’re averting real jail time,” says Dr. Fred Osher, director of health systems and services policy at the Council of State Governments Justice Center, a nonprofit that consults on public safety issues.
Copyright 2015 Kaiser Health News. To see more, visit Kaiser Health News.
Read Original Article – December 16, 2015 11:10 AM ET
One approach to battling addiction and other behavioral health issues lies just outside our front doors. (Photo by Theresa Soley/KTOO)
Police reports, the press and social media are flooded with stories of substance abuse, heroin overdoses and deaths in Alaska’s capital.
One approach for battling addiction and other behavioral health issues lies just outside our front doors.
“Across the world people seek solitude or wilderness experiences because there is a healing process,” said Jerrie Dee, clinical director at Alaska Crossings.
Alaska Crossings is a wilderness therapy program for youth with behavioral issues, including those with a history of drug abuse. The program takes adolescents, ages 12-18, on 64-day canoe trips into wild Southeast from Wrangell.
The program uses wilderness as a catalyst for healing, Dee said. Natural challenges, silence and a sacred process emerge when immersed in the outdoors. Dee said these things can redirect someone’s life.
Dee said wilderness immersion gives recovering drug users an opportunity to reset because external triggers and temptations are not present in the outdoors.
“Often times substance use is more an emotional process than it is physical,” she said.
Using surveys before, during and after immersion, Alaska Crossings has documented a substantial decline in participants’ negative symptoms. Long term effects after leaving the wilderness are harder to measure.
Dee said the process works for adults, too, but as far as she knows, there aren’t any wilderness therapy programs for people over 18 in Alaska.
Larry Olson, a licensed master addiction counselor in Juneau, said that many of the patients he sees started using prescription drugs in high school. With time, the habits spiraled into full addictions. He said there is no formula; some of his patients come from rough homes, but many come from loving families.
Most of the six people who died of heroin overdoses in Juneau since February were under the age of 30, according to Alaska Dispatch News. And Olson said a large portion of his patients are under 30.
Alaska Crossings admits youth who have struggled with addiction, but it is not a drug treatment program. Dee said that in the wilderness, guides can’t monitor for health issues, including withdrawal.
When substance abuse is an applicant’s primary issue, it must be treated before admittance to Alaska Crossings and entering the wilderness, Dee said.
This two-tier theory, detox then therapy, is common for wilderness addiction treatment programs.
Olson, the addiction counselor, said that many adults who are battling addiction have weak, deteriorated bodies. High levels of activity may not be an option.
But Olson said less rigorous wilderness experiences could provide opportunities for healing. He said that many of his patients speak of the importance of nature in their personal spirituality. Rekindling the human relationship with the natural world can be very healing, he said.
“If people can redevelop a sense of awe and wonder at just life, that is really very, very good,” he said.
The program follows a three-step process. The first is to develop discipline and routine, next is a focus on the participant’s unique treatment ambitions and third is learning to apply new skills to everyday life at home, said Alaska Crossings Director Stephen Helgeson.
Helgeson said that paying for wilderness therapy programs, both as an organization and for participants, is the greatest challenge. Lack of funding makes it difficult to provide help to those who need it most.
He hopes that as Medicaid expansion develops, more funding will become available for low-income adults.
Close
Update notification options
Subscribe to notifications
Subscribe
Get notifications about news related to the topics you care about. You can unsubscribe anytime.




9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))


9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))


9(MDEwMjQ0ODM1MDEzNDk4MTEzNjU3NTRhYg004))
